
Contents of Article
- Summary
- What is Heart Rate Variability (HRV)?
- How is Heart Rate Variability used to determine recovery status?
- Does Heart Rate Variability affect performance?
- How is Heart Rate Variability affected by training?
- Is Heart Rate Variability valid and reliable?
- Is future research needed with Heart Rate Variability?
- Conclusion
- References
- About the Author
Summary
The interest in heart rate variability (HRV) appears to be growing year on year, particularly as technology develops and our ability to quickly establish a reliable measure using a smartphone improves. HRV reflects the variation in time between each heartbeat, otherwise known as the R–R interval or the inter-beat interval. Whilst HRV-guided training appears to be more effective for developing aerobic performance than pre-planned training, it does not appear to be a reliable predictor of overreaching – but this has been scrutinised by methodological issues within the research.
HRV has been shown to be a predictor of illness in elite athletes, but its ability to predict injury is yet to be validated in humans. The use of modern technology such as smartphone applications, heart rate monitors, and finger-wave pulse sensors have been shown to be a reliable measure of HRV.
Lastly, HRV can be accurately measured during ultra-short durations (one minute), and be done so in either a supine, seated, or standing position.

What is Heart Rate Variability (HRV)?
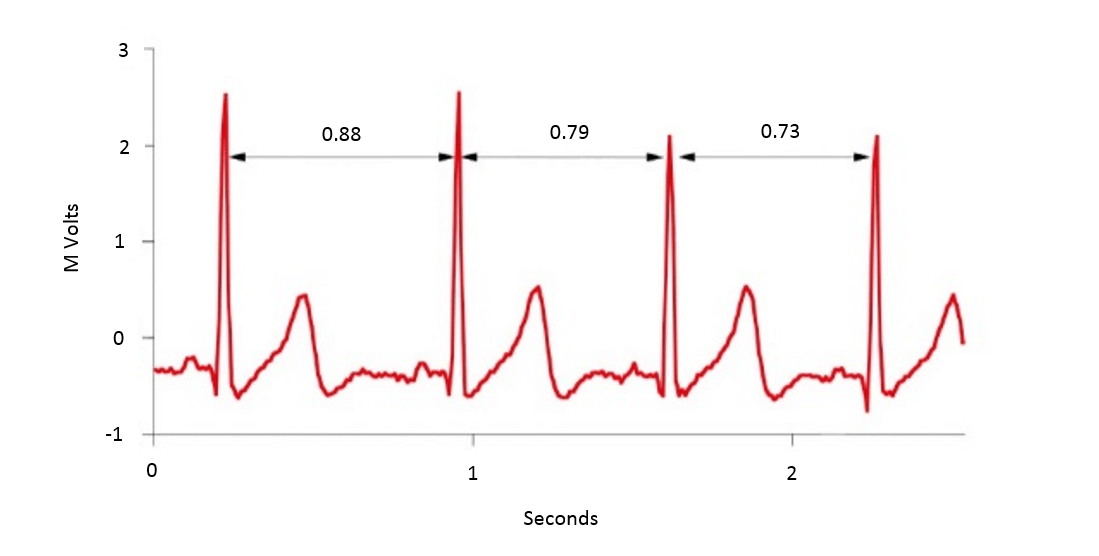
Heart rate variability (HRV) is simply the time difference between each successive heartbeat, otherwise known as the R–R interval or the inter-beat interval (Figure 1). The time between each heartbeat is not fixed/consistent, it varies with every beat – hence the term heart rate ‘variability’.
The term heart rate variability (HRV) appears to become more and more popular as continued research into this metric keeps identifying its association with athletic performance and recovery (1). On top of this, there are now many HRV tracking apps available for simple daily monitoring using a smartphone (2).
Historically, HRV has been measured using an electrocardiogram (ECG), but with the development of technology, it can now be reliably measured using smartphone applications combined with a heart rate strap (3), or a finger-wave pulse sensor (4). Whilst there are many other metrics used to measure HRV, the most common and perhaps reliable is technically known as the ‘root-mean-square difference of successive normal R–R intervals (RMSSD)’ (5). Thus in practical sporting environments, HRV is most frequently measured using the RMSSD metric. Two other common HRV metrics used within sports science are high-frequency power (HFP), and the standard deviation of instantaneous beat-to-beat R–R interval variability (SD1) (6).
Aside from the importance of HRV in athletic performance, its main significance is its use in the medical environment. That is, HRV has been shown to be a predictor of mortality after a heart attack (7, 8), and is also related to congestive heart failure (9), diabetic neuropathy (10, 11, 12), depression (13, 14), post-cardiac transplant (15), susceptibility to sudden infant death syndrome (SIDS) and poor survival in premature babies (16).
How is Heart Rate Variability used to determine recovery status?
This is where things get a little more complicated, but we have attempted to keep it as short and informative as possible.
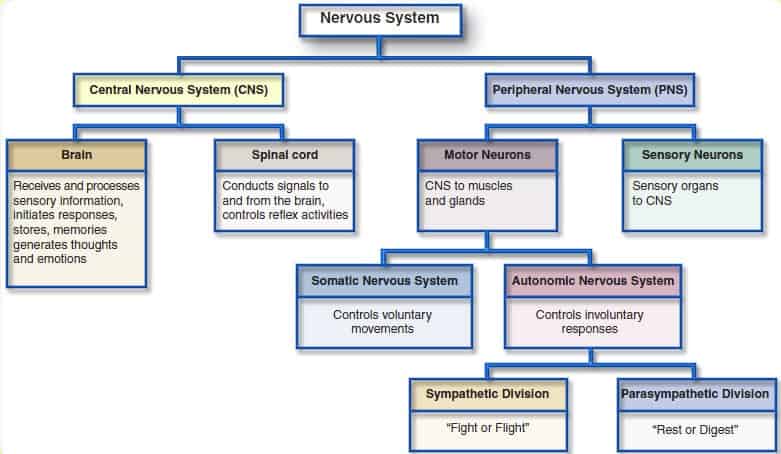
Firstly, and this is important to remember, the variability in your heart rate (i.e. HRV) provides critical information about the function of your autonomic nervous system (ANS), and it is also the most reliable measurement of ANS function (10). An increase in HRV represents a positive adaptation/better recovery status, whilst a reduction in HRV reflects stress and worse recovery status. Having said that, it is important to note that higher is not always better, and lower is not always worse (17) – but that is beyond the scoop of this article. But as a golden rule of thumb, the higher the athlete’s HRV, the fitter/better recovered they are, and vice versa. The ANS is comprised of two branches, these are the sympathetic nervous system (SNS) and the parasympathetic nervous system (PSNS) (Figure 2).
The easiest way to distinguish the differences between these two branches is to associate “fight or flight” responses with the SNS, and “rest and digest” responses with the PSNS. Therefore, the SNS increases heart rate and the PSNS slows it down – this can be seen in Figure 3.
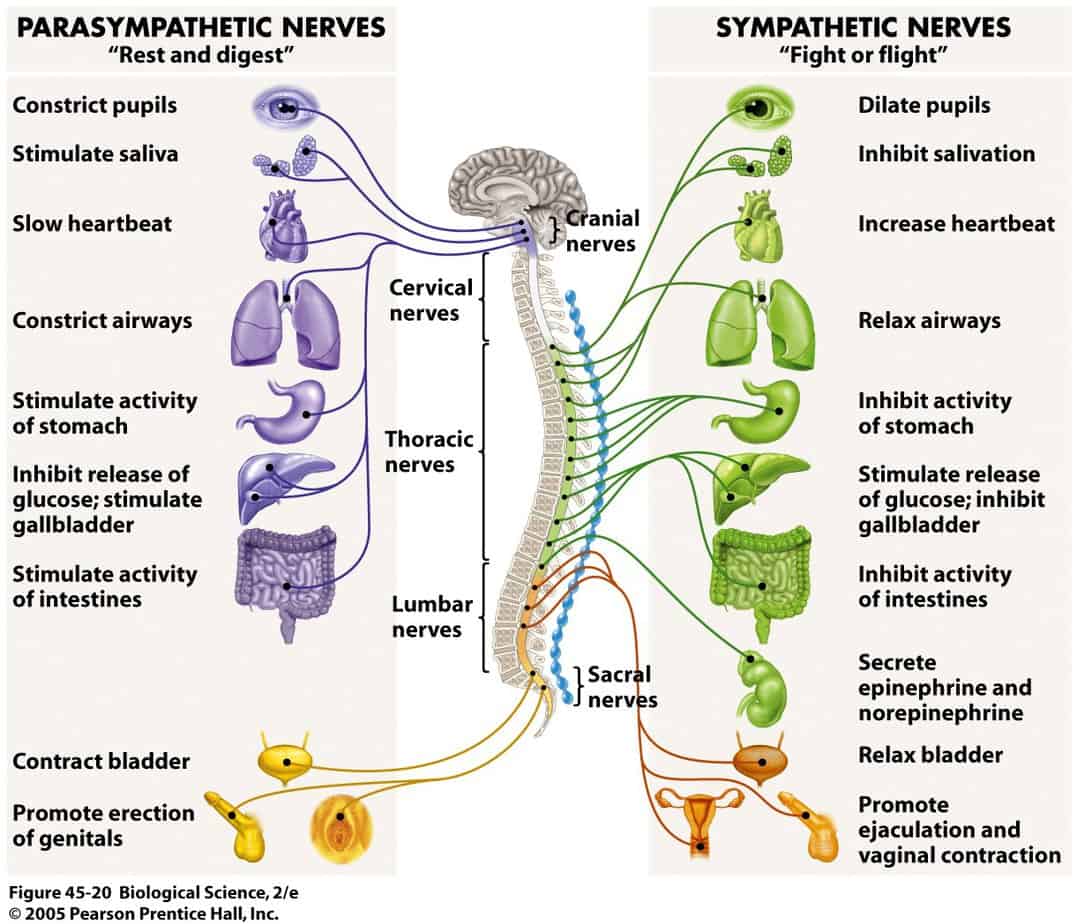
So, the SNS is responsible for “exciting” the body in stressful environments (e.g. competition) and does so by stimulating the responses seen in Figure 3. For example, one of which is by stimulating the secretion of adrenaline and noradrenaline; otherwise known as epinephrine and norepinephrine, these hormones prepare the body for stress. More relevantly, the SNS also increases heart rate, force of contraction, and blood pressure, leading to an increased blood flow to the muscles (18). Therefore, anytime you or your athlete has felt an “adrenaline rush” before a competition, this is essentially your SNS being stimulated and preparing you for competition.
On the flip side, the PSNS does the complete opposite and is responsible for reducing heart rate and blood pressure in the absence of stress. Essentially, the PSNS helps facilitate recovery after a stressful event (e.g. competition) by counteracting the effects of the SNS (18).
Put simply then, the SNS increases heart rate and blood flow to the muscles, whilst the PSNS reduces heart rate and peripheral blood flow – in effect, they counteract one another. However, both are essential for performance and recovery. The SNS stimulates the body for the stressors experienced during performance, and the PSNS is vital for recovery and regeneration. It is believed that an “imbalance” between the SNS and PSNS can lead to reductions in athletic performance, and in more extreme cases, lead to overtraining (19).
To add to this, HRV is also affected by mental and chemical stress as well as physical stress. For example, mental stressors such as job/work-related stress (20), making complex decisions (21), public speaking tasks (21), and performing tests/exams (22, 23) have all been shown to significantly reduce HRV. In fact, one study reported that athletes experiencing high levels of stress make smaller strength gains than those with lower stress levels (24). In addition, chemical stressors such as alcohol have been repeatedly shown to reduce HRV (25, 26, 27, 28, 29).
As HRV can accurately measure ANS function (balance between SNS and PSNS) and can do so in a non-invasive manner, it is commonly used by exercise scientists to monitor systemic fatigue and recovery. Having the ability to monitor an athlete’s systemic recovery status, of course, has its “pros” and “cons”. The “pros” mean the coach can identify the athlete’s recovery status on a comprehensive scale which includes physical, mental, and chemical stress; other than wearable technology (GPS) which only displays physical/external stress. Whilst the “cons” mean the coach cannot be exact with which one of those stressors (physical, mental, or chemical) is causing the highest amount of stress to the athlete – but perhaps this is where the coach-athlete interaction and the wellness questionnaires play their part.
Does Heart Rate Variability affect performance?
As HRV reflects ANS function and thus stress, it is frequently used in the athletic world to identify periods of optimal training and to monitor recovery status and any potential overtraining (30). It has been suggested that monitoring HRV can help identify the following:
- Accurately reflect recovery status (19).
- Help determine if an athlete is overtraining (19).
- Identify when the athlete may be more or less adaptive to training (aiding training prescription) (19).
- Potentially predict when an athlete may perform better or worse on a particular day (19).
- Potentially predict when the athlete is more susceptible to illness or injury (31, 32).
Though some of these claims are rather substantial, there is a firm body of research to support a number of them (21, 30, 33, 6).
HRV and Recovery Status
A number of research studies have highlighted a reduction in HRV following intense training sessions. One, in particular, observed a reduction in HRV 24 hours post-workout following a high-intensity strength training session. HRV and weightlifting performance returned to baseline (i.e. pre-workout values) after 72 hours of recovery, indicating a relationship between HRV and recovery (34). Another study also found a relationship between training load and HRV before and during rowing World Championships in national rowers (35).
They reported when the athletes were subjected to high training loads leading up to competition, their HRV dropped significantly. Once training loads were substantially lowered during competition, their HRV then increased and returned to baseline. Another study that monitored athletes over a long period of time (multiple months) found that HRV increased during an intense training period, but then stagnated and lowered during an overload training phase. But after a two-week recovery period, HRV rebounded and even led to an increase in HRV (36). This also indicates that intense training regimes may even improve HRV.
HRV and Overreaching
Though HRV has been reported to be a reliable marker of overreaching, two recent reviews may not support this theory. A 2016 systematic review and meta-analysis has suggested that resting HRV is largely unaffected by overreaching – i.e. HRV cannot identify overreaching – but they also suggested this may be the result of methodological issues that require further investigation (6). This study agrees with a previous review which also reported that resting HRV may not necessarily correlate with overreaching (33).
HRV and Performance
When discussing HRV and its effects on performance, the concept of HRV-guided training versus pre-planned training is often analysed. HRV-guided training simply refers to prescribing each training session based on the athlete’s HRV score. For example, if the athlete’s HRV is normal or higher than normal, then they will be prescribed an intense training session. Alternatively, when the athlete’s HRV is below normal, then they are prescribed an easier, lower-intensity session. Pre-planned training simply refers to a programme that has already been designed and does not cater for daily changes in HRV.
A 2007 study compared the effects of HRV-guided training against pre-planned training. The authors reported the HRV-guided training group improved running performance (maximal running velocity) more than the pre-planned group (37). In support of this study, another more recent investigation also found HRV-guided training in males to be more effective than pre-planned training (38). Interestingly, however, they did not see the same improvements in females. However, the female HRV-guided training group who performed fewer high-intensity training sessions still experienced parallel performance gains to the pre-planned group. Furthermore, other research found a relationship between athletes who had high HRV scores and improved VO2max, compared to those who had low HRV scores and showed deterioration in VO2max performances (39).
All in all, this suggests that HRV-guided training may be more beneficial for improving aerobic performance when compared to pre-planned training regimes. It also suggests that athletes who have a higher HRV score may be more sensitive to performance gains than those with a lower HRV score. Important to note, there is no research to our knowledge that demonstrates that HRV-guided training is more effective for strength development than pre-planned training – the research only supports aerobic development.
HRV and Illness or Injury
To date, there is little research identifying any relationships between HRV and illness or injury. In fact, to the best of our knowledge, there is only one study to date that has displayed a link between HRV and illness in elite swimmers (i.e. upper respiratory tract and pulmonary infections) (40).
In regards to HRV being a predictor of injury, one unpublished study conducted on horses – another mammal – displayed a relationship between HRV and both injury and illness (31). Another study which is currently under the data collection phase is attempting to identify a relationship between HRV and overuse injuries in humans (32). The authors believe that HRV monitoring has the potential to reveal the influence of external stimuli such as fatigue, nutrition, and stress on the recovery and protection of damaged somatic tissue.
How is Heart Rate Variability affected by training?
Without going into too much detail and getting too technical, as it is beyond the scope of this article, we will briefly elaborate on how HRV is thought to be affected by performance.
The increase in parasympathetic modulation (i.e. the PSNS ability to modulate/control its functions, reducing heart rate for example) and HRV is the result of the classical physiological adaptations typically shown following endurance training interventions. Put briefly, endurance training causes a volume load on the heart, which in turn leads to an increase in left ventricular internal dimension and wall thickness, and in end-diastolic volume (due to increased plasma volume and decreased peripheral resistance), ultimately leading to an increase in stroke volume.
An increased stroke volume means a decreased heart rate can maintain the same cardiac output (at least at rest and during sub-maximal exercise). This leads to a decreased metabolic load on the heart, creating a more efficient time-pressure relationship. The decrease in resting heart rate is due in part to an increase in parasympathetic modulation, which is consequently reflected in an increase of HRV (6).
Is Heart Rate Variability valid and reliable?
HRV has been shown to be a valid and reliable predictor of ANS function (10). Moreover, other than electrocardiograms (ECG), more practical methods of measuring HRV such as heart rate straps (3) and finger-wave pulse sensors (4) have also been shown to be valid and reliable. To add to this, even some particular brands such as Polar® have even had their watches proven to be valid and reliable measures of HRV (41, 42, 43). Other research has also validated the use of certain technologies such as the Omega Wave System (43) and even smartphone applications (3).
When monitoring HRV in athletic training plans, an interesting and growing metric being used instead of RMSSD to measure acute and chronic fluctuations in recovery status is the coefficient of variance. However, this will not be discussed in any more detail within this article.
Age/Population
Current research suggests that HRV is a very reliable measure of ANS function in adults (1, 44, 45, 46). Intra- and inter-daily measures of HRV also appear to be very reliable in elite athletes (47). However, there appears to be conflicting evidence with the research on children (6-12 years); with some suggesting it is reliable (48, 49), and others suggesting it is not (50, 51). Future research on the validity and reliability of HRV in children is therefore vital.
Duration
Traditionally, it took 10 minutes to obtain an accurate HRV measure (five minutes of stabilisation followed by five minutes of recording), but with progressions in both research and technology, ultra-short recordings are now possible. Ultra-short recordings of just one minute are capable of providing reliable measures of HRV (47, 52, 53, 54, 3)
Position
It is possible to reliably measure ultra-short HRV recordings (1 minute) in the following positions:
- Supine (54, 3, 55, 53)
- Seated (47, 53)
- Standing (53)
Is future research needed with Heart Rate Variability?
As this metric continues to grow its reputation as an effective marker of recovery status and a potential marker of illness and injury, more research should be directed towards understanding its true potential. This means future research projects should aim to identify:
- Relationships between HRV and illness.
- Relationships between HRV and injury.
- HRV-guided training for strength and power development.
- The effects of acute and chronic HRV monitoring on performance.
- Whether athletes are more susceptible to performance gains when HRV is high.
- Reliability of HRV in children.
- Whether HRV accurately reflects recovery status in various sporting populations (e.g. endurance, strength/power, team sport athletes’) and in other varying populations (males, females, geriatric and paediatric).
Conclusion
- HRV reflects the variation in time between each heartbeat.
- Low HRV scores are associated with many forms of disease.
- HRV appears to correlate with recovery status.
- Resting HRV does not appear to reliably reflect overreaching.
- Athletes with high HRV scores may perform better on endurance-based tests
- Athletes with higher stress levels may make smaller strength gains.
- HRV-guided training appears to induce greater performance gains than pre-planned training programmes.
- HRV may be a useful predictor of illness (i.e. upper respiratory tract and pulmonary infections).
- HRV may be a predictor of injury risk, but this is yet to be validated by any research on humans.
- HRV is increased by improving the time-pressure relationship of the heart.
- Technologies such as Polar® watches and the Omega Wave System appear to produce reliable HRV readings.
- HRV can be measured during ultra-short recordings (one minute) and during standing, seated, or supine positions.

- Pinna GD, Maestri R, Torunski A, Danilowicz-Szymanowicz L, Szwoch M, La Rovere MT, Raczak G. Heart rate variability measures: a fresh look at reliability. Clin Sci (Lond). 2007 Aug;113(3):131-40. [PubMed]
- Best heart rate variability apps in ios (Top 100) – AppCrawlr. 2016. Best heart rate variability apps in ios (Top 100) – AppCrawlr. [ONLINE] Available at: http://appcrawlr.com/ios-apps/best-apps-heart-rate-variability. [Accessed 29 May 2016].
- Flatt AA, and Esco MR. Validity of the ithleteTM Smart Phone Application for Determining Ultra-Short-Term Heart Rate Variability. Journal of Human Kinetics volume 39/2013, 85-92. [PubMed]
- Heathers JAJ. Smartphone-enabled pulse rate variability: An alternative 2 methodology for the collection of heart rate variability in 3 psychophysiological research. Int J Psychophysiol. 2013 Sep;89(3):297-304. [PubMed]
- Aubert AE, Seps B, and Beckers F. (2003). Heart Rate Variability in Athletes. Sports Med 2003; 33 (12): 889-919. [PubMed]
- Bellenger CR, Fuller JT, Thomson RL, Davison K, Robertson EY, Buckley JD. Monitoring Athletic Training Status Through Autonomic Heart Rate Regulation: A Systematic Review and Meta-Analysis. Sports Med, Ahead of Print. [PubMed]
- Bigger JT Jr; Fleiss JL; Steinman RC; Rolnitzky LM; Kleiger RE; Rottman JN. (1992). “Frequency domain measures of heart period variability and mortality after myocardial infarction”. Circulation. 85 (1): 164–171. [PubMed]
- Kleiger RE, Miller JP, Bigger JT Jr, Moss AJ (1987). “Decreased heart rate variability and its association with increased mortality after acute myocardial infarction”. Am J Cardiol. 59 (4): 256–262. [PubMed]
- Bilchick KC, Fetics B, Djoukeng R, Fisher SG, Fletcher RD, Singh SN, Nevo E, Berger RD. Prognostic value of heart rate variability in chronic congestive heart failure (Veterans Affairs’ Survival Trial of Antiarrhythmic Therapy in Congestive Heart Failure). Am J Cardiol. 2002 Jul 1;90(1):24-8. [PubMed]
- Risk M, Bril V, Broadbridge C, Cohen A. Heart rate variability measurement in diabetic neuropathy: review of methods. Diabetes Technol Ther. 2001 Spring;3(1):63-76. [PubMed]
- Chessa M, Butera G, Lanza GA, Bossone E, Delogu A, De Rosa G, Marietti G, Rosti L, Carminati M.. Role of heart rate variability in the early diagnosis of diabetic autonomic neuropathy in children. Herz. 2002 Dec;27(8):785-90. [PubMed]
- Pagani M. Heart rate variability and autonomic diabetic neuropathy. Diabetes Nutr Metab. 2000 Dec;13(6):341-6. [PubMed]
- Nahshoni E, Aravot D, Aizenberg D, Sigler M, Zalsman G, Strasberg B, Imbar S, Adler E, Weizman A. Heart rate variability in patients with major depression. Psychosomatics. 2004 Mar-Apr;45(2):129-34. [PubMed]
- Agelink MW, Boz C, Ullrich H, Andrich J. Relationship between major depression and heart rate variability. Clinical consequences and implications for anti-depressive treatment. Psychiatry Res. 2002 Dec 15;113(1-2):139-49. [PubMed]
- Cornelissen, VA, Vanhaecke J, Aubert AE, Fagard RH. Heart rate variability after heart transplantation: A 10-year longitudinal follow-up study. Journal of Cardiology Volume 59, Issue 2, March 2012, Pages 220–224. [Link]
- Antila KJ, Välimäki IA, Mäkelä M, Tuominen J, Wilson AJ, Southall DP. Heart rate variability in infants subsequently suffering sudden infant death syndrome (SIDS). Early Hum Dev. 1990 May;22(2):57-72. [PubMed]
- Freelap USA. 2016. Interpreting HRV Trends in Athletes: High Isn’t Always Good and Low Isn’t Always Bad – Freelap USA. [ONLINE] Available at: https://www.freelapusa.com/interpreting-hrv-trends-in-athletes-high-isnt-always-good-and-low-isnt-always-bad/. [Accessed 08 June 2016].
- Tortora, G.J., and Derrickson, B.H. (2009). Principles of Anatomy and Physiology. Volume 1, 12th ed. John Wiley & Sons: Asia. [Link]
- Flatt AA. HRVtraining. 2016. Heart Rate Variability Explained: Part 1 | HRVtraining. [ONLINE] Available at: https://hrvtraining.com/2012/01/16/heart-rate-variability-explained-part-1/. [Accessed 01 June 2016].
- Vandeput, S, Taelman J Spaepen A, and Van Huffel S. Heart Rate Variability as a Tool to Distinguish Periods of Physical and Mental Stress in a Laboratory Environment. [Link]
- Dong GJ. The role of heart rate variability in sports physiology. Exp Ther Med. 2016 May; 11(5): 1531–1536. [PubMed]
- Taelman J, Vandeput S, Spaepen A, and Van Huffel S. Influence of Mental Stress on Heart Rate and Heart Rate Variability. Eur J Appl Physiol. 2004 Jun;92(1-2):84-9. [PubMed]
- Hjortskov N, Risse´n D, Blangsted AK, Fallentin N, Lundberg U, Søgaard K. The effect of mental stress on heart rate variability and blood pressure during computer work. Eur J Appl Physiol (2004) 92: 84–89. [Link]
- Bartholomew, JB, Stults-Kolehmainen, MA, Elrod,CC, and Todd, JS. Strength gains after resistance training: the effect of stressful, negative life events. J Strength Cond Res 22: 1215–1221, 2008. [PubMed]
- P.F.D. et al. (2011) Acute ingestion of alcohol and cardiac autonomic modulation in healthy volunteers. Alcohol, 45: 123-9. [PubMed]
- Koskinen, P. et al. (1994) Acute alcohol intake decreases short-term heart rate variability in healthy subjects. Clinical Science, 87(2): 225-30. [PubMed]
- Sagawa,Y. et al. (2011) Alcohol has a dose-related effect on parasympathetic nerve activity during sleep. Alcoholism: Clinical & Experimental Research, 35(11): 2093-99. [PubMed]
- Spaak, J. et al. (2009) Dose-related effects of red wine and alcohol on heart rate variability. American Journal of Physiology, Heart & Circulatory Physiology, 298(6): H2226-31. [PubMed]
- Weise, F. et al. (1986) Acute alcohol ingestion reduces heart rate variability. Drug & Alcohol Dependence, 17(1): 89-91. [Link]
- Aubert AE, Seps B, Beckers F. Heart rate variability in athletes. Sports Med. 2003;33(12):889-919. [PubMed]
- Ross, C. What’s at the heart of breakdowns? Equus;May 2008, Issue 368, p46. [Link]
- Gisselman AS, Baxter GD, Wright A, Hegedus E, Tumilty S. Musculoskeletal overuse injuries and heart rate variability: Is there a link? Med Hypotheses. 2016 Feb;87:1-7. [PubMed]
- Bosquet L, Merkari S, Arvisais D, Aubert AE. Is heart rate a convenient tool to monitor over-reaching? A systematic review of the literature. Br J Sports Med. 2008 Sep;42(9):709-14. [PubMed]
- Chen, J-L, Yeh, D-P, Lee, J-P, Chen, C-Y, Huang, C-Y, Lee, S-D, Chen, C-C, Kuo, TBJ, Kao, C-L, and Kuo, C-H. Parasympathetic nervous activity mirrors recovery status in weightlifting performance after training. J Strength Cond Res 25(6): 1546–1552, 2011. [PubMed]
- IELLAMO, F., F. PIGOZZI, A. SPATARO, D. LUCINI, and M. PAGANI. T-Wave and Heart Rate Variability Changes to Assess Training in World-Class Athletes. Med. Sci. Sports Exerc., Vol. 36, No. 8, pp. 1342–1346, 2004. [PubMed]
- PICHOT, V., T. BUSSO, F. ROCHE, M. GARET, F. COSTES, D. DUVERNEY, J. R. LACOUR, and J. C. BARTHE´LE´MY. Autonomic adaptations to intensive and overload training periods: a laboratory study. Med. Sci. Sports Exerc., Vol. 34, No. 10, pp. 1660–1666, 2002. [PubMed]
- Kiviniemi, A.M., Hautala, A., Kinnumen, H., & Tulppo, M. (2007) Endurance training guided by daily heart rate variability measurements. European Journal of Applied Physiology, 101: 743-751. [PubMed]
- Kiviniemi, A.M., Hautala A.J., Kinnunen, H., Nissila, J., Virtanen, P., Karjalainen, J., & Tulppo, M.P. (2010) Daily exercise prescription on the basis of HR variability among men and women. Medicine & Science in Sport & Exercise, 42(7): 1355-1363. [PubMed]
- Hedelin, R., Bjerle, P., & Henriksson-Larsen, K. (2001) Heart Rate Variability in athletes: relationship with central and peripheral performance. Medicine & Science in Sports & Exercise, 33(8), 1394-1398. [PubMed]
- HELLARD, P., F. GUIMARAES, M. AVALOS, N. HOUEL, C. HAUSSWIRTH, and J. F. TOUSSAINT. Modeling the Association between HR Variability and Illness in Elite Swimmers. Med. Sci. Sports Exerc., Vol. 43, No. 6, pp. 1063–1070, 2011. [PubMed]
- Giles D, Draper N, Neil W. Validity of the Polar V800 heart rate monitor to measure RR intervals at rest. Eur J Appl Physiol. 2016; 116: 563–571. [PubMed]
- NUNAN, D., G. DONOVAN, D. G. JAKOVLJEVIC, L. D. HODGES, G. R. H. SANDEROCK, and D. A. BRODIE. Validity and Reliability of Short-Term Heart-Rate Variability from the Polar S810. Med. Sci. Sports Exerc., Vol. 41, No. 1, pp. 243–250, 2009. [PubMed]
- Parrado E, García MA, Ramos J, Cervantes JC, Rodas G, Capdevila L. Comparison of Omega Wave System and Polar S810i to detect R-R intervals at rest. Int J Sports Med. 2010 May;31(5):336-41. [PubMed]
- Sookan, T. Heart rate variability in physically active individuals: reliability and gender characteristics. Cardiovasc J Afr. 2012 Mar; 23(2): 67–72. [PubMed]
- Warren JH, Jaffe RS, Wraa CE, Stebbins CL. Effect of autonomic blockade on power spectrum of heart rate variability during exercise. Am J Physiol. 1997 Aug;273(2 Pt 2):R495-502. [PubMed]
- Cottin F, Papelier Y, Escourrou P. Effects of exercise load and breathing frequency on heart rate and blood pressure variability during dynamic exercise. Int J Sports Med. 1999 May;20(4):232-8. [PubMed]
- Nakamura FY, Pereira LA, Esco MR, Flatt AA, Moraes JE, Abad CCC, Loturco I. Intra- and inter-day reliability of ultra-short-term heart rate variability in rugby union players. J Strength Cond Res. 2016 May 25. [Epub ahead of print]. [PubMed]
- McNarry MA, Mackintosh KA. Reproducibility of Heart Rate Variability Indices in Children with Cystic Fibrosis. PLoS One. 2016 Mar 11;11(3):e0151464. [PubMed]
- Seppälä S, Laitinen T, Tarvainen MP, Tompuri T, Veijalainen A, Savonen K, Lakka T. Normal values for heart rate variability parameters in children 6-8 years of age: the PANIC Study. Clin Physiol Funct Imaging. 2014 Jul;34(4):290-6. [PubMed]
- Winsley RJ, Armstrong N, Bywater K, Fawkner SG. Reliability of heart rate variability measures at rest and during light exercise in children. Br J Sports Med. 2003 Dec;37(6):550-2. [PubMed]
- Leicht AS, Allen GD. Moderate-term reproducibility of heart rate variability during rest and light to moderate exercise in children. Braz J Med Biol Res. 2008 Jul;41(7):627-33. [PubMed]
- Esco MR and Flatt AA. Ultra-short-term heart rate variability indexes at rest and post-exercise in athletes: evaluating the agreement with accepted recommendations. J Sports Sci Med 13: 535-541, 2014. [PubMed]
- Flatt AA and Esco MR. Heart rate variability stabilization in athletes: towards more convenient data acquisition. Clin Physiol Funct Imaging In Press, 2015. [PubMed]
- Esco MR, Flatt AA, Wellborn B, Nakamura NY. Agreement between a smart-phone pulse sensor application and ECG for determining lnRMSSD. J Strength Cond Res. 2016. [Link]
- Flatt AA, Esco MR, Nakamura FY, Plews DJ. Interpreting daily heart rate variability changes in collegiate female soccer players. J Sports Med Phys Fitness. 2016 Mar 11. [PubMed]

