
Contents of Article
- Summary
- Why is recovery important in sports?
- What is cold water immersion?
- Does cold water immersion improve recovery?
- How does cold water immersion improve recovery?
- Acute vs. chronic cold water immersion
- Are there any issues with cold water immersion?
- What future research is needed with cold water immersion?
- Tips for using cold water immersion
- References
- About the Author
Summary
Cold water immersion therapy is becoming an increasingly popular recovery protocol and has been proven to improve recovery for subjective measures, but its effects on objective measures are far less apparent. Despite its ability to improve recovery, the underpinning psycho-physiological responses of this recovery method are still not fully understood.
Whilst further research is needed, the attenuation of inflammatory pathways and the hydrostatic effects of water immersion both pose interesting concepts for the positive effects of cold water therapy. Furthermore, plunging into cold water may be less beneficial in terms of recovery than immersion into thermoneutral water temperatures. The chronic effects of cold water immersion are still not fully understood, but some research has suggested that it may hinder vascular and muscular adaptations from both endurance and resistance training. Lastly, a recent study has reported that the optimal immersion duration is between 11-15 minutes.
Why is recovery important in sports?
Recovery is a critical part of training as it is used to minimise the risk of overtraining and injury, whilst promoting physical and psychological readiness. This becomes particularly important during intense training or competition periods to sustain an optimal state of performance (1). Understanding its importance has led to the use and development of many recovery techniques such as massage therapy, foam rolling, electrical stimulation, whole-body vibration, compression garments, hyperbaric oxygen therapy and water immersion therapy (including cold water, warm water, and contrast bathing).
For its ability to improve recovery time and reduce the delayed onset of muscle soreness (DOMS), water immersion therapy has become a popular recovery method amongst sports scientists (2, 3). The term water immersion therapy generically refers to all modes of water-based recovery protocols – namely cold-water immersion, warm-water immersion, and contrast bathing (alternate warm and cold immersion). It is commonly believed that water immersion therapy can:
- Reduce oedemas
- Decrease the perception of pain associated with muscular soreness
- Decrease the perception of fatigue
- Alter localised blood flow
- Alter localised tissue and core temperature
- Alter heart rate
- Reduce muscle spasms
- Reduce tissue inflammation
- Reduce muscle damage
- Improve range of motion
However, whilst some research may support some of these effects, others have little, to no evidence supporting these assumptions.
What is cold water immersion?
Cold water immersion (CWI), otherwise known as ice-baths, plunges pools and cold water therapy, is a recovery process involving the immersion of the body into cold water (≤ 15 ˚C/59 ˚F) immediately after exercise in an attempt to enhance the recovery process (2). Despite being shown to only have a small impact on recovery, CWI has proven to be an effective method for enhancing recovery (2, 3, 4).
Does cold water immersion improve recovery?
Depending on the intensity, exercise can cause various degrees of fatigue to the musculoskeletal, nervous, and metabolic systems. Exercise is also associated with microscopic tears in muscle tissue, commonly known as exercise-induced muscle damage (EIMD), this can then cause DOMS (2, 3).
The effectiveness of CWI has been investigated by measuring several factors. These include:
Subjective Measures
- DOMS (Delayed Onset of Muscle Soreness) (3)
- Ratings of Perceived Exertion (RPE) (3)
Objective Measures
- Creatine-kinase (CK) (3)
- Blood lactate levels (3)
- Interleukins (3)
- C-reactive protein (CRP) (3)
In a large quantity of research, CWI has been shown to consistently reduce the effects of DOMS and RPE. In a recent systematic review and meta-analysis, it was concluded that CWI is an effective protocol for reducing the effects of DOMS 24 hrs (hours), 48 hrs, and 96 hrs post-exercise (3). Moreover, it was also shown to reduce the symptoms of RPE 24 hrs post-exercise (3). These results are also supported by an extensive review conducted by Bleakley et al. (2012) (2).
Whilst numerous research supports the use of CWI for reducing the effects of subjective measures post-exercise (i.e. DOMS and RPE), its effects on objective measures are far less apparent (3). If CWI fails to improve objective measures of recovery (listed above), then this raises questions about the mechanisms responsible for reducing the effects of DOMS and RPE.
How does cold water immersion improve recovery?
Despite there being an abundance of research on CWI, the primary mechanisms for its ability to improve recovery are still not fully understood. However, the following theories have been suggested:
- Vasoconstriction (blood vessel constriction).
- Analgesic (pain relieving) effect of the cold water.
- Reducing inflammatory pathways.
- Placebo effect.
- Hydrostatic pressure.
Vasoconstriction
One theory suggests that immersion into cold water causes vasoconstriction, leading to lower localised blood flow (5). It is thought the cold temperature activates the thermal nerve cells (nociceptors), leading to a change in sympathetic nerve activity and is therefore responsible for this reduced blood flow. The temperature-induced reduction in blood flow around the damaged tissues, caused by strenuous exercise, reduces oedemas and inflammatory activity (6, 7).
Analgesic effects of cold water
The second theory postulates the reduced perception of pain is due to the analgesic effect of cold water. Whereby immersion into cold water leads to decreased nerve conduction speeds and excitability (8), thus reducing nociceptor communication with the sympathetic nervous system (9, 10, 11). Ultimately, this would lead to a reduction in the perception of pain.
Reducing inflammatory pathways
Others have suggested the decrease in the perception of pain is related to reduced inflammatory pathways – namely: reduced nociceptor sensitisation (12), reduced exercise-induced oedema (13), and reduced white blood cell access (2, 14). This theory is, therefore, a combination of effects, and is often referred to in the research as the primary physiological reason for improved recovery.
Placebo effect
Another theory suggests that the effectiveness of CWI on the reduction of post-exercise pain and fatigue is primarily down to psychological perception (i.e. a placebo effect). This suggests the individual simply feels more ‘awake’ during and/or after the immersion into the cold water, causing a decrease in their sensitivity to pain (2, 15). This theory is supported by a recent and extensive review conducted by Hohenauer et al. (2015) (3), who reported that CWI reduces the athlete’s perception of DOMS and RPE.
Hydrostatic pressure
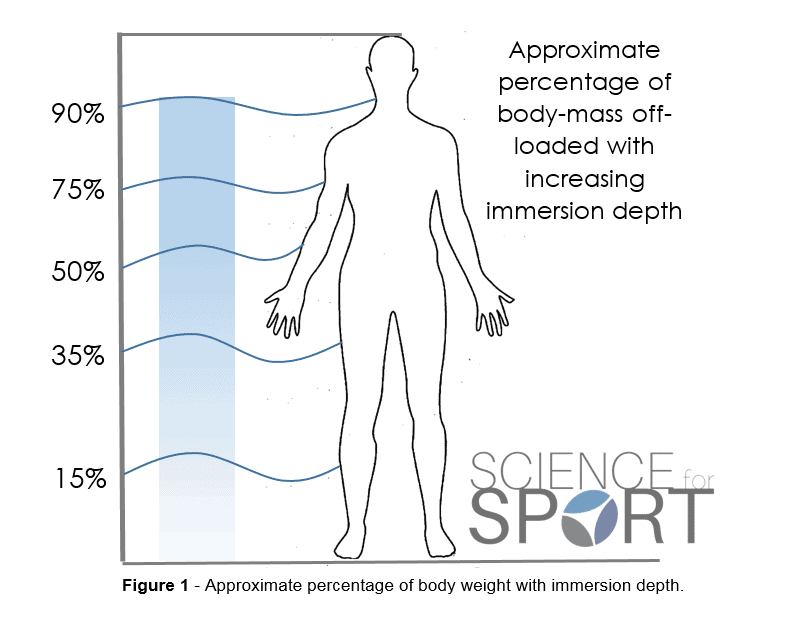
Another theory lies with the effects of hydrostatic pressure on the body during immersion into water. When an individual is immersed in water they are subject to the effects of hydrostatic pressure. For every 1-metre of immersion, the pressure gradient rises by 74 millimetres of mercury (mm Hg) – this is almost equal to typical diastolic blood pressure (80 mm Hg) (9). As the pressure gradient increases with depth (i.e. the deeper you go, the more pressure imposed), this hydrostatic pressure causes an inward and upward squeezing action on the body. It is this mechanism that causes the effects of buoyancy. The buoyancy reduces the gravitational load on the body, meaning objects such as the human body weigh less when in water. Figure 1 demonstrates the reduction in body weight at various water immersion depths.
During immersion at hip level, the hydrostatic pressure causes the displacement of fluids from the lower extremities of the body towards the thoracic region. Some experts believe the movement of these fluids towards the thoracic region may be the principal component for enhanced recovery (9). It is thought that this action may reduce exercise-induced oedemas, increases the transfer of extracellular fluid into the bloodstream and increases cardiac output (9). Increased cardiac output means increased blood flow and metabolism of waste products that accumulate during exercise. The buoyancy effect of water immersion may also reduce fatigue by lowering neuromuscular signalling and improving energy conservation (9).
Interestingly, immersing athletes in water that is too cold may actually counteract some of the positive effects caused by the hydrostatic pressure. Colder water induces vasoconstriction, reducing heart rate and thus cardiac output. This response causes the body to reduce peripheral blood flow and preserve its core temperature, as a result, central metabolism is increased in order to maintain this core temperature (9).
The increased central metabolism enhances the production of waste products and erodes energy stores, both of which are considered negative and unwanted effects after exercise and when attempting to enhance recovery time (9). As a result, it is suggested that perhaps immersion in cool-to-thermoneutral water temperatures* may be the best option for recovery, unless muscles strain or sprains have occurred, in which case immersion into colder temperatures may be more beneficial (9).
*The water temperature of 34-35 ˚C (93-95 ˚F) is known as the thermoneutral zone, the ambient temperature range in which a person, who is at rest and healthy, neither shivers nor sweats.
Acute vs. chronic cold water immersion
As it is believed that CWI speeds-up short-term (acute) recovery by reducing inflammatory pathways, one of the greatest current debates with regards to using CWI is whether using this modality on a continuous basis reduces long-term (chronic) adaptations in physical development (e.g. strength, hypertrophy etc). In other words, does using CWI after every, or most, training sessions and matches reduce vascular and muscular adaptations?
Though there is not a great deal of research on this topic, some of the current research does suggest that continual use of CWI can reduce vascular and muscular adaptations from both endurance and resistance training (17, 18, 19). Having said this, other conflicting studies suggest that continual CWI has no negative effects on chronic adaptations (20, 21). The current uncertainty within research simply means that it is still unclear whether continuous CWI use reduces long-term adaptations or not.
If the continual use of CWI does hamper chronic adaptations, then this may suggest that they may only be worthwhile during intense training/competition periods, and not during regular schedules. On another note, this also questions the necessity for non-professional athletes who only train and compete approximately 2-3 times per week, and who do not have intense training/competition schedules where the primary goal is performance maintenance, rather than performance enhancement. However, all of these are questions yet to be answered.
Are there any issues with cold water immersion?
Availability
A common problem with CWI is the accessibility and/or transportability of ice baths. Official ice baths are often expensive pieces of equipment which require an abundance space for usage, which can be difficult for non-professional teams due to lack of funds and available space. This led to the improvisation of other resources as replacements, such as wheelie bins and paddling pools.
Lack of knowledge
Understanding the primary mechanisms responsible for the recovery-enhancing effects of CWI would lead to improved practical application. For example, if it was solely identified that CWI was purely a placebo effect modality and that thermoneutral water immersion was most effective, then practitioners could simply raise the water temperature. Using thermoneutral temperatures would increase involvement/compliance in water immersion therapy as many athletes often avoid CWI due to discomfort and/or a dislike of the recovery method.
Duration of immersion
Within the current body of research, there is a substantial variation in the immersion durations, with times ranging from 1-15 minutes (2, 3), and no common agreement in optimal time being achieved. Interestingly, a 2016 systematic review of the current research has identified that durations of between 11-15 minutes provide the best results for cold water immersion (22). It has also been recorded that it takes approximately 10 minutes for the movement of interstitial-intravascular fluid to occur, suggesting that immersion should be of at least 10 minutes in order to optimise the effects of recovery – which at thermoneutral temperatures is very achievable.
What future research is needed with cold water immersion?
Whilst there is an abundance of research on CWI, there are still large discrepancies within the information and the chosen methodologies. Consequently, much greater exploration is needed in order to advance current knowledge and enhance the effectiveness of this recovery method. Some needed areas of research include:
- Investigating optimal water temperatures (e.g. CWI vs thermoneutral water therapy).
- Analgesic effect of CWI.
- Dose-response relationships: Optimal duration of immersion and/or repeated immersion (sets) and the magnitude of recovery.
- Optimal depth of immersion.
- Effects on diverse populations (e.g. gender, youth, elderly, sporting level).
- Chronic effects of CWI.
- Optimal timing of post-exercise CWI (e.g. 1, 5, 15, 60 minutes)
Tips for using cold water immersion
Temperature
Although there is currently no agreed temperature for optimal results, temperatures from research typically range between 8-15 ˚C (46-59 ˚F) with a mean temperature of 11 ˚C (52 ˚F) (4). Consequently, it is therefore advised that practitioners use temperatures of approximately 11˚C (52 ˚F) in an attempt to capitalise upon any effect caused by lower (8 ˚C/46 ˚F) or higher (15 ˚C/59 ˚F) temperatures used during CWI.
Duration
Current research suggests the optimal immersion duration is between 11-15 minutes. Moreover, to ensure the occurrence of blood plasma fractioning (movement of interstitial-intravascular fluid), it is suggested that individuals remain immersed for at least 10 minutes in an attempt to optimise the effects of recovery. However, it is understood that immersion of this duration is relatively impractical, particularly when working with large teams. As the positive effects of CWI have been reported using durations of 1-15 minutes (2, 3), then practitioners may opt for shorter durations despite the unknown advantages or disadvantages.
Immersion depth
As the hydrostatic pressure may be an important factor in recovery (9), it is suggested that the deeper the athlete is immersed, the higher the potential for improvement. In addition, as the objective of immersion is to move fluids from the periphery towards the thoracic region and immersion imposes an inward and upward force on the body, it is generally advised that athletes remain upright during immersion. However, this may vary depending upon the sport or activity – i.e. upper-limb dominant sports may find added benefit from being immersed in the supine position.
Conclusion
Whilst cold water immersion is commonly used in practical environments, still very little is known about the best protocols to use in order to optimise recovery. There is also still disagreement on the optimal temperature to induce maximal recovery effects, in addition to an ever-increasing knowledge of thermoneutral water temperatures – which may appear more effective than cold water. In summary, vertical full-body immersion into cold (≤ 15 ˚C/59 ˚F) to thermoneutral temperatures 34-35 ˚C (93-95 ˚F) for 11-15 minutes post-exercise appears to have a positive effect upon recovery.

- Mair SD, Seaber AV, Glisson RR, Garrett WE (1996). The Role of Fatigue in Susceptibility to Acute Muscle Strain Injury. American Journal of Sports Medicine.24:137–143. [PubMed]
- Bleakley, C., McDonough, S., Gardner, E., Baxter, G.D., Hopkins, J.T., & Davison, G.W. (2012). Cold-water immersion (cryotherapy) for preventing and treating muscle soreness after exercise. Cochrane Database Syst Rev. 15(2). CD008262. [PubMed]
- Hohenauer E, Taeymans J, Baeyens J-P, Clarys P, Clijsen R (2015) The Effect of Post-Exercise Cryotherapy on Recovery Characteristics: A Systematic Review and Meta-Analysis. PLoS ONE 10(9): e0139028. doi:10.1371/journal.pone.0139028 [PubMed]
- Bieuzen, F., Bleakley, C.M., and Costello, J.T. (2013). Contrast Water Therapy and Exercise Induced Muscle Damage: A Systematic Review and Meta-Analysis. PLoS One, 8(4): e62356. [PubMed]
- Gregson, W., Black, M.A., Jones, H., Milson, J., and Morton J. (2011). Influence of cold water immersion on limb and cutaneous blood flow at rest. American Journal of Sports Medicine, 39: 1316–1323. [PubMed]
- Lee, H., Natsui, H., Akimoto, T., Yanagi, K., Ohshima, N. (2005). Effects of Cryotherapy after Contusion Using Real-Time Intravital Microscopy. Medicine and Science in Sports and Exercise, 37: 1093–1098. [PubMed]
- Thorlacius, H., Vollmar, B., Westermann, S., Torkvist, L., Menger, M.D. (1998). Effects of local cooling on microvascular hemodynamics and leukocyte adhesion in the striated muscle of hamsters. J Trauma, 45: 715–719. [PubMed]
- Algafly AA, George KP (2007) The effect of cryotherapy on nerve conduction velocity, pain threshold and pain tolerance. Br J Sports Med 41: 365–369; discussion 369. [PubMed]
- Wilcock, I.M., Cronin, J.B., and Hing, W.A., (2006). Physiological response to water immersion: A method of recovery? Sports Medicine, 36(9), pp.747-765. [PubMed]
- Eston R, Peters D (1999) Effects of cold water immersion on the symptoms of exercise-induced muscle damage. J Sports Sci 17: 231–238. [PubMed]
- Coffey V, Leveritt M, Gill N (2004) Effect of recovery modality on 4-hour repeated treadmill running performance and changes in physiological variables J Sci Med Sport 7: 1–10. [PubMed]
- Kuligowski LA, Lephart SM, Giannantonio FP, Blanc RO (1998). Effect of whirlpool therapy on the signs and symptoms of delayed-onset muscle soreness. J Athl Train 33: 222–228. [PubMed]
- Kraemer WJ, Bush JA, Wickham RB, Denegar CR, Gomez AL, et al. (2001) Influence of compression therapy on symptoms following soft tissue injury from maximal eccentric exercise. J Orthop Sports Phys Ther 31: 282–290. [PubMed]
- Clarkson PM, Hubal MJ (2002) Exercise-induced muscle damage in humans. Am J Phys Med Rehabil 81: S52–69. [PubMed]
- Leeder J, Gissane C, van Someren K, Gregson W, Howatson G (2012) Cold water immersion and recovery from strenuous exercise: a meta-analysis. Br J Sports Med 46: 233–240. [PubMed]
- Torres-Ronda, L., & del Alcázar, X. S. i. (2014). The Properties of Water and their Applications for Training.Journal of Human Kinetics, 44, 237–248. [PubMed]
- Yamane M, Teruya H, Nakano M, Ogai R, Ohnishi N, Kosaka M. Postexercise leg and forearm flexor muscle cooling in humans attenuates endurance and resistance training effects on muscle performance and on circulatory adaptation. Eur J Appl Physiol 2006; 96: 572–580. [PubMed]
- Yamane M, Ohnishi N, Matsumoto T. Does Regular Post-exercise Cold Application Attenuate Trained Muscle Adaptation? Int J Sports Med 2015; 36: 647–653. [PubMed]
- Frohlich, M, Faude, O, Klein, M, Pieter, A, Emrich, E, and Meyer, T. Strength training adaptations after cold-water immersion. J Strength Cond Res 28(9): 2628–2633, 2014. [PubMed]
- Halson, S.L., Quod, M.J., Martin, D.T., Gardner, A.S., Ebert, T.R. & Laursen, P.B. (2008) Physiological responses to cold water immersion following cycling in the heat. International Journal of Sports Physiology and Performance. Vol. 3, No. 3: 331–46. [PubMed]
- Ihsan M, Markworth JF, Watson G, Choo HC, Govus A, Pham T, Hickey A, Cameron-Smith D, Abbiss CR. Regular postexercise cooling enhances mitochondrial biogenesis through AMPK and p38 MAPK in human skeletal muscle. Am J Physiol Regul Integr Comp Physiol. 2015 Aug 1;309(3):R286-94. [PubMed]
- Machado AF, Ferreira PH, Micheletti JK, Almeida AC, Lemes IR, Vanderlei FM, Junior JN, Pastre CM. Can Water Temperature and Immersion Time Influence the Effect of Cold Water Immersion on Muscle Soreness? A Systematic Review and Meta-Analysis. Sports Med (2016) 46:503–514. [PubMed]

