
Contents
- Summary
- Introduction
- Overview of the nature of injuries in grappling sports
- Mechanism of Injury (MOI)
- Risk Factors
- Barriers & Facilitators of introducing injury prevention warm-up
- Appraising evidence for warm-up intervention protocols
- Conclusion
- Appendix
- References
Summary
Grappling sports are becoming more popular, but with this injuries associated with grappling sports are on the rise. At present, no injury prevention warm-up (IPW) specifically addresses the requirements of grappling athletes. Using existing guidelines and frameworks from other sports and disciplines, this article proposes an IPW to meet the specific needs of the grappling athlete.
Introduction
Greco-Roman wrestling has been featured in the Olympic games since they started in 1896, with Catch wrestling being introduced in 1904 before being replaced by Freestyle wrestling in 1924. Regardless of the long history of the three sports, no injury-prevention warm-up has been published (1) despite poor warm-ups previously being cited as a common cause of injury in grappling sports (2). Additionally, there is currently no injury prevention warm-up (IPW) for other grappling sports such as Brazilian jiu-jitsu (BJJ) and Sambo.
Overall injury rates for grappling sports can be up to 19.6 per 1000 hours of athlete exposure (AE) (3), with competition rates reaching 109 injuries/1000 AE (4). High injury recurrence rates have also been highlighted in grappling sports (5). Research has shown that the successful employment of warm-ups before sports can reduce athlete injury and recurrence rates (6, 7, 8).
The Team-Sport Injury Prevention (TIP) cycle is a revised version of Flinch’s (2006) Translating Research into Injury Prevention Practice Framework (TRIPP). `TIP details the process of development of an evidence-based injury prevention programme. TIP identifies stages of designing an injury prevention programme as; (re)evaluate, identify, and intervene (9) (Figure 1).
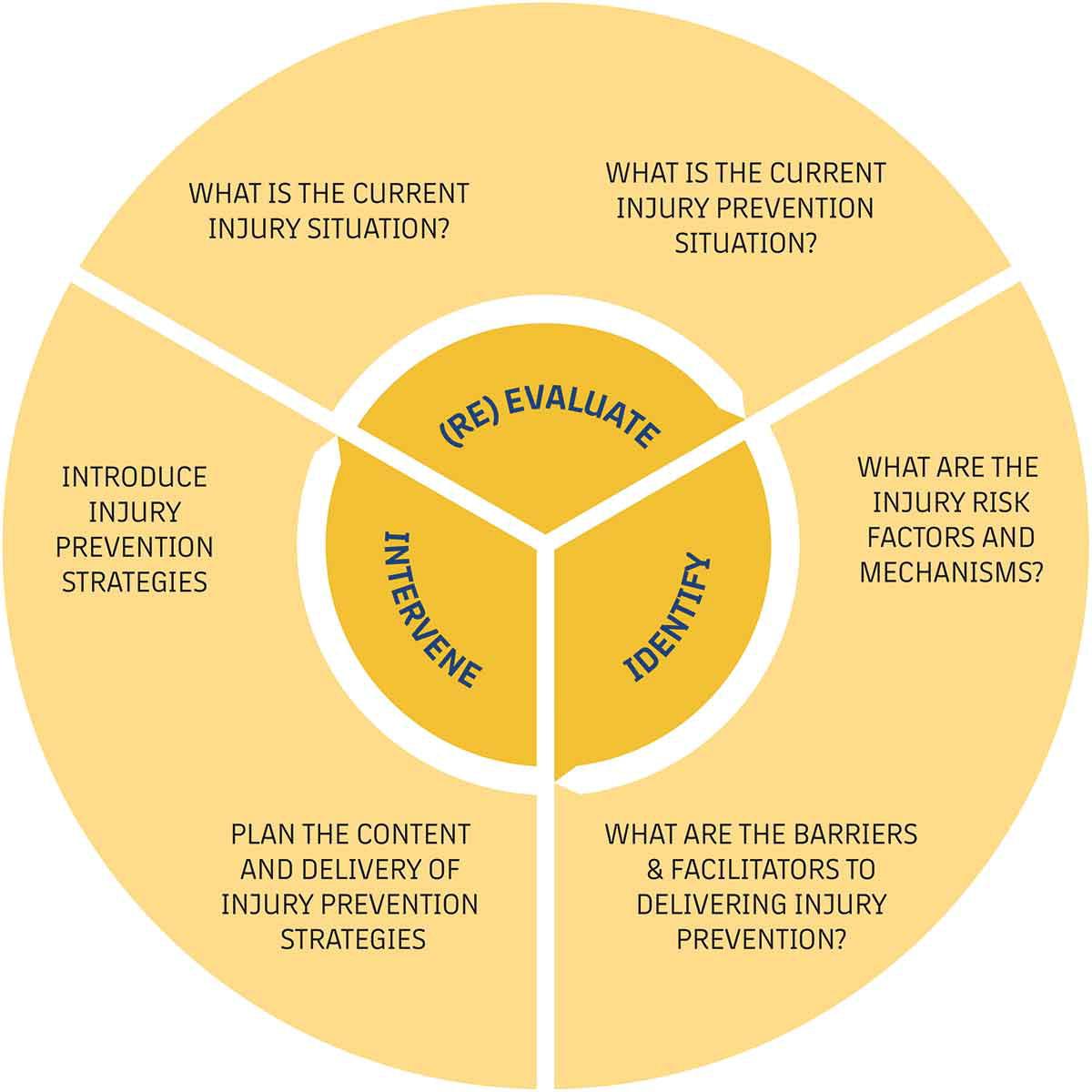
Figure 1. The Team-Sport Injury Prevention (TIP) cycle is a revised version of Flinch’s (2006) Translating Research into Injury Prevention Practice Framework (TRIPP) (9).
This review proposes an evidence-based injury prevention warm-up intervention to reduce injury incident rates in grappling sports. It will discuss the sites and types of injuries seen in wrestling, BJJ and Sambo, and the mechanism of injury (MOI) and barriers to delivery of an injury prevention warm-up. The approach to developing the IPW was to first assess the available research to establish the current injury situation in grappling sports, including the nature and frequency of injuries. Followed by the barriers and facilitators of introducing an injury prevention warm-up. Once the appraisal of the research literature was complete, an IPW was designed with the input of grappling researchers and practitioners.
Overview of the nature of injuries in grappling sports
Incidence of injury
There are multiple injury surveillance data studies available for Freestyle wrestling. However, the injury incident rate (IR) does differ between samples, with overall IR being as low as 3.40 per 1000 hours of athlete exposure (AE) in British wrestlers (10) to 19.6 injuries/ 1000 AE seen in American collegiate male wrestlers (3). There is a paucity of published injury surveillance data for BJJ. However, two studies do report competition injury incident reporting rates ranging from 9.2 to 24.9 injuries/ 1000 AE (11. 12). This is much lower than rates seen in freestyle wrestling competitions, where rates range from 13.1 to 42.01/ 1000 AE (10, 13, 14, 15, 16).
Anatomical site of injuries and Type
Multiple Injury studies in BJJ have established that the Knee is the most commonly injured anatomical site, ranging between 20.8 to 81.1 % of all injuries occurring (5, 11, 12, 17, 18, 19, 20, 21). Two studies found hands and fingers to be the most frequent injuries in BJJ, followed by the Knee (22, 23, 24). In BJJ competitions the elbow was the most commonly injuries joint. However, the Knee had the highest incidence of medical diagnoses (11). None of the grapplers stated if injuries came from Gi-based BJJ or No-Gi BJJ. The head, neck and trunk were the leading injury sites present at American Emergency Departments for BJJ between 2008 to 2015 (25). BJJ Studies that reported injury type stated sprains as the leading diagnosis (21, 24, 26).
In several American collegiate wrestling injury surveillance studies, the Knee has been reported as the most frequent injury in competition and practice (16.7 % to 30.4 %) (3, 13, 14, 16, 27). However, this differs in American high school wrestlers, where the head/face (practices = 19.9 %, competitions = 21.4 %) and shoulder/clavicle (practices = 14.1 %, competitions = 21.0 %) were the most common injury sites (16). Data obtained from various demographics has established knee strains/sprains as the most frequent injury wrestlers (14, 28, 29).
There are still grappling arts with no research data available, such as Catch Wrestling. Others, such as Sambo and Japanese jiu-jitsu, have limited research. Blach et al. (2022) (30) Joint study of spinal injuries in Sambo reported that 53 % of all reported spinal injuries occurred in the lumbar region. In traditional Jiu-jitsu, the knee (29.4 %) (31) is stated as the most frequent injury site, while minor contusions, sprains, and muscle injuries (54 %) were the leading injury type (32).
Greco-Roman studies often show differences in the leading injury sites varying from the Neck, Ribs and Shoulder (33, 34, 35). In competition lactations to the face are the leading injury site and type (62%) (36). Mooren et al. (2023) (37) systematic review of Injuries during Judo Tournaments stated that the majority of studies reported the Head and Neck as the leading injury site. The leading time loss injury site was the knee, and the leading injury type was joint sprains followed by contusions and lacerations. Anterior cruciate ligament (ACL) ruptures have been reported as the primary injury type for time loss with 32 % of all ACLs taking 6-9 months for grapplers to return to play (38).
The review of the available research shows that the knee is the most commonly injured site in Freestyle wrestling (3, 13, 14, 16, 27), BJJ (5, 11, 12, 17, 18, 19, 20, 21) and traditional Jiu-jitsu (31) and the leading time loss injury in Judo (37, 38). Ligament strains were reported as the leading injury type in Freestyle wrestling, BJJ (21, 24, 26) and Judo (37) and second in traditional Jiu-jitsu (32). In Greco-Roman Wrestling and Judo competitions, the grappling sports that do not allow leg attacks, the head, neck and trunk are the leading injury sites (33, 34, 35, 36, 37).

Mechanism of Injury (MOI)
Freestyle wrestling research is unanimous in stating that takedowns were the leading MOI, resulting in 39 % to 54.3 % of all reported injuries (10, 13, 14, 16, 27, 39). The majority of these happened during practice sparring 37.5 % to 65.1 % (10, 13, 14, 27). This was also seen in BJJ, where studies reported that 74-77.6 % of injuries happened during training (17, 21). It was also established that submissions (29.7 %) were the leading MOI, followed by takedowns (26.4 %). An opponent attempting an armbar was the leading submission to cause injury, and the triangle submission was the leading cause of injury for grapplers attempting a submission on their opponent (17). The MOI has also been shown to differ between ages with one study reporting the leading MOI for adolescents as Tumbling/ Trauma and takedowns as the lead MOI for adults and masters (40). In BJJ competitions, the armbar was the most common MOI (28.8 %), followed by takedowns (13.9 %) (11).
Sandeep and Haridas Kuloor’s (2017) (35) study of Greco-roman wrestlers states that most injuries accrued with contact with the opponent. However, it does not go any further as to what the contact was or why it occurred. A systematic review of competition injuries in Judo found that 50 to 85.2 % of injuries happened during Tachi-waza (Standing techniques) (37). The most frequent method of MOI in standing techniques is being thrown, followed by performing a throw then grip fighting (41, 42, 43). The available research shows that takedowns and throws are the leading aetiology in all styles of wrestling and Judo, with BJJ research fluctuating between takedowns and submissions.
Risk Factors
Compared to many sports physical risk factors in grappling is under-researched. However, some studies may help the design of the IPW. In youth freestyle wrestling a relationship has been found between reduced flexibility and an increased rate of skeletal and muscular-tendinous injuries (44). A link between bone injuries and isometric strength was also established (44). In Judo and BJJ interlimb asymmetries in strength, power and flexibility in the knee, shoulder and hip have been associated with injury risk (45, 46). In Judo breakfall techniques are heavily researched (47). Although no injury incident or prevalence studies exist, ample studies show that grapplers who show incorrect falling techniques demonstrate poor collision biomechanics associated with head and neck injuries (47). Practicing correct falling techniques has been shown to lower these dysfunctions (47).
Research has highlighted multiple factors that contribute to increased injury risk. Studies have shown that injury incident rates increase with age in BJJ, Freestyle wrestling and Judo (10, 17, 37, 48, 49). Multiple BJJ studies have shown females to be at greater risk of injury (5, 40). However, studies in Freestyle and Judo have presented mixed results for gender injury incident rates (37, 50). Grappling experience and training volume have also been established as risk factors (10, 26, 40, 48). However, studies have shown that grapplers with more experience train more times a week and for longer durations (49) meaning that the increased injury incident rates in experienced grapplers may come from increased training volume.
Although research into risk factors is lacking in grappling sports the available studies suggest that strength, power, and flexibility affect injury incident and prevalence rates. The decline in these physical attributes seen with age may be the reason that injury incident rates increase with age (51, 52). An exercise selection with evidence of increasing strength, power and flexibility will be included in the IPW.
Armbars and Upper-body injury
One of the leading MOIs in BJJ is the armbar (11, 17). The armbar is a submission that involves grapplers hyperextending their opponent’s elbow joint by inflicting a posterior-to-anterior (P/A) force to the humerus and an anterior-to-posterior (A/P) force to the forearm (53, 54). Almeida et al. (2017) (54) study on the patterns and mechanisms of armbar injuries stated that force caused by the eccentric contraction of the forearm flexor muscles, leading to injury of the dynamic and static medial stabilisers of the elbow. The chances of dislocation and distal humerus shear fractures expand as the valgus moment increases when the elbow is at full extension (55, 56). Due to the level of force that can be produced, it is unlikely that the IPW will have any impact in reducing injuries from armbars; instead, sparring etiquette and the correct paring of sparring partners with similar weight and experience levels.
The head and neck are leading injury sites in Judo and Greco-Roman wrestling with the direct impact of the head on the mat being stated as a frequent MOI (47). Research in the elucidation of the causes of head injury in judo has shown that grapplers landing from unexpected throws (eyes closed) exhibited greater maximum angular acceleration of the head compared to expected throws (eyes open) (57). The delayed reaction to a push and delayed contraction of the neck muscles has also been linked to the increased risk of head injury (57). It was also seen that anterior cervical flexion strength had no impact on angular acceleration (57). Research on the Ukemi break-fall technique has shown that it can dramatically reduce peak resultant translational acceleration of the head that is associated with an acute subdural haematoma and coronal rotation that has been linked to diffuse axonal injury (58, 59, 60).
Research into neck strengthening exercises in the sport of Rugby Union and Mixed martial arts has shown a reduction in cervical muscle injuries and sports-based concussions (61, 62). Neck strength has been associated with Peak Angular Momentum of Neck Extension (PAMNE) (47). PAMNE is lower in experienced judoka when compared to novices when performing break-falls (63). As neck strength was not tested in the study it is unclear if PAMNE was lower due to better break-fall technique or from neck strength. It appears necessary to include both break-fall drills and neck strengthening exercises in the IPW.
Leg attacks and Lower-body injury
Takedowns have been verified as the most utilised method for scoring points in competitions and are therefore practised regularly in grappling sparring and drilling (64, 65, 66). It has been established that many BJJ, freestyle, and catch wrestling takedowns, most noticeable leg attacks, involve knee torsion, lateral knee displacement and excessive force transmitted in the joint in the execution phase (67, 68, 69). Research in ACL and injuries states that the primary kinetic mechanisms are valgus forces, compressive anterior force of the quadriceps, and short axial compressive forces to the knee that cause anterior translation of the tibia (39). These variables contribute to the most frequent component of ACL strain, proximal tibia anterior shear (70, 71). The MCL is commonly injured through coronal plane impact merged with rotational forces (72, 73). The kinetic forces seen in pivoting movement, rapid deceleration, and forced hyperextension are chief mechanisms in combined knee ligament injuries (74).
These MOI align with the mechanisms of leg-based takedowns frequently performed in BJJ and Various types of wrestling. Additionally, it has been observed that freestyle wrestlers rely predominantly on leg attacks and not throws, as seen in Greco-Roman wrestling and Judo (64, 75). This is due to rulesets, as it is not permitted to grab the legs in Greco-roman wrestling and Judo. This has led to different defence strategies and postures between grappling styles that can attack the legs and those that cannot. Grappling styles that permit leg attacks, such as BJJ, freestyle and catch wrestling, demonstrate greater A/P excursion of the centre of pressure and greater knee flexion that results in significantly increased joint angles in the transverse and frontal planes at the knee and ankle due to the lowered stance needed to attack and defence the lower limbs (42, 76). This may contribute to the higher percentage of knee and lower limb injuries and higher injury prevalence rates seen in freestyle wrestling (34, 36, 77).
As suplexes are not permitted in BJJ (78), it can be presumed that the majority of takedowns are attacks to the legs and not throws, as seen in Greco-Roman wrestling and Judo (33, 37). This leads to the conclusion that grappling sports that allow leg attacks share similar MOI and can be separated from those that are not permitted to perform leg attacks. Unlike technique drilling for head injuries and coaching advisement for submission injuries there are many IPW that are designed to lower injuries to the knee joint. Research has shown that knee-focused IPW can successfully lower injuries in contact sports (79,80). Exercises from these IPW that are most relevant to grappling, can be included in the current IPW.
Current recommendations to reduce injury
Grindstaff & Potach (2006) (81) reviewed wrestling injuries and suggested exercises to be incorporated into a strength and conditioning (S&C) programme. This resource is useful for S&C coaches and provides a framework for a gym-based injury prevention programme. However, many of the exercise suggestions involved gym equipment that would not be possible to use for a team warm-up. However, some bodyweight exercises, such as wheelbarrow holds and bear crawls, may be adapted to fill a warm-up format. Von Gerhardt et al. (2023) (82) designed an injury-prevention warm-up for Judo called the Injury Prevention and Performance Optimization Netherlands (IPPON). It is the only published injury prevention warm-up tailored for a grappling sport. However, it focused purely on the injuries and MOIs seen in Judo. However, the IPPON intervention did not significantly reduce the overall and severe injury prevalence.
Injury prevention warm-ups have successfully reduced injury rates and precursors to injury in sports such as Football, Basketball and rugby (83, 84, 85, 86). Following a similar systematic evidence-based approach as these programs have previously, an effective injury prevention warm-up protocol for grappling arts may be designed.

Barriers & Facilitators of introducing injury prevention warm-up
Barriers to Injury Prevention
There are some frequently reported barriers to compliance with injury prevention programmes in sport. The Minnig et al. (2022) (87) review of the barriers to the adoption of evidence-based injury prevention programmes states perceived time, financial cost, coaches lacking confidence in their ability to implement it, and the inclusion of exercises that were difficult or confusing to follow. Studies that were not included in the review stated similar barriers such as not knowing what to do, not having been previously injured, not having the correct equipment and a lack of knowledge from coaches on how to implement the programme (88, 89, 90).
Facilitators of Injury Prevention
Research on the barriers and facilitators of injury prevention programmes has stated coach education is a major contributor to improving compliance (89, 90, 91). The British Wrestling Association (BWA) has agreed to act as a facilitator for the injury prevention programme. This encompasses embedding IPW into the British wrestling coaching course, as seen in FIFA coaching licence courses and the FIFA 11+ IPW. The BWA will also make the IPP warm-up available as an online continuous professional development course (CPD) for international grappling coaches.
To overcome other barriers such as lack of time (87, 90), costs (92), scheduling (93), and equipment (89) the IPW is designed to last 15 to 20 mins and will take place at the start of scheduled training sessions or completions. The IPW will not need any equipment and can be implemented by coaches to minimise the cost of hiring S&C coaches or physiotherapists. It has been stated that athletes and coaches perceive performance increases as a higher motivation than injury prevention (94). Research has shown that associating injury prevention programmes with increased performance benefits increases compliance rates (95, 96, 97). Due to this, the IPW will be designed in the Raise, Activate/ Mobilise and Potentiate (RAMP) (98) structure will be used as it was designed to optimise performance preparation (98). The IPW also includes Plyometric and Post-activation Potentiation Enhancement (PAPE) techniques that have been shown to increase athletic performance (96, 97, 99).
Appraising evidence for warm-up intervention protocols
Duration and protocol
A frequently reported barrier to injury prevention programmes is perceived time and scheduling (87, 90, 93), so keeping the IPW protocol compact is a requirement that may help with compliance from coaches and grapplers. A 2016 systematic review on the effect of team warm-ups by Silva et al. (2018) (100) found that a warm-up protocol of 15 minutes was the optimal period to increase explosive performance. In terms of reducing injury kinematic and kinetic dysfunctions associated with injury risk factors and reduced injury incidence, several IPWs lasting between 15 to 20 minutes have been shown to be effective (101, 102, 103, 104, 105, 106). Studies have shown a compliance rate of a minimum of 2 times a week is needed for IPW of this duration to be successful (101, 106, 107, 108).
The RAMP warm-up protocol has been successfully used in combat and contact sports such as Rugby league and boxing (99, 109). The rationale for the activities included in the IPW is formatted in the structure of the RAMP protocol.
Raise
The raise section aims to elevate body temperature, heart rate, respiration rate, blood flow, and joint fluid viscosity via low-intensity activities (98). Reviews have shown that effective warm-up protocols increase the intensity until a heart rate similar to that of a competitive environment is reached (100). Research has recorded an average heart rate of 180 to 182 bpm in grappling matches and can reach a maximum of 190 – 200 (110, 111). Exercises such as high knees, heels to glutes, and head rolls have increased dynamic mobility of the spine and peripheral joints (84). Meanwhile, rolling has been shown to increase proprioception and postural control (112, 113). Additionally, Grapplers need the ability to produce a rate of force development (RFD) and acceleration for movements such as takedowns (69). Shuffle sprints will help with the RFD (114) and aid in increasing HR.
Activate
The activate section focuses on identifying the key muscles needed for grappling and then using a selection of dynamic movements to activate them (115). The physical demands of grappling involve all major muscle groups (116, 117). This section of the IPW will start with walking lunges with trunk rotation. EMG research has demonstrated that forward lunges increased activation in the Vastus Mediali and gluteus Medius and have been used in peer-reviewed injury prevention and performance warm-ups (118, 119, 120). The lunges will be followed by bear crawls, which have been used in wrestling and functional training settings to activate the wrists, pelvis and lower limbs (121, 122). Sports-specific movements have been shown to be effective in previous injury prevention programmes (123). The wheelbarrow position mimics wrestling positions that require the grappler to support their body weight with their upper extremities (81). Research using EMG has shown that press-up variations such as the wheelbarrow exercise activated the lower trapezius and the serratus anterior (124). Press-ups have been demonstrated to increase upper body and core activation (125, 126, 127) and have been used effectively in injury prevention warm-ups (128). Hindu press-ups involve a significant degree of trunk and hip flexion that mimics the 110 degrees of trunk/hip flexion seen in the biomechanical analysis of a sprawl (129).
Much like the Hindu press-up, Hindu squats are commonly used in various wrestling styles. The squat has been successfully used to lower injury prevention and increase performance in the FIFA 11 + protocol (8, 130). The Hindu squat also allows grapplers to move into greater degrees of knee flexion needed to perform movements such as the double leg takedown (147 degrees) (129). Research has shown that many head, neck and trunk injuries in BJJ are a result of landing (25). It has been recommended that increased training in landing techniques will aid in preventing landing and fall injuries as previously demonstrated in Judo (25, 47, 63). Short-term breakfall practice has been shown to improve electromyography (EMG) activity in Stenocleidomastoid, External Oblique and Rectus Abdominis muscles (131).
Mobilise
The lack of mobility has been acknowledged as an injury precursor in grappling sports (17). Additionally, it has been shown that grappling requires athletes to exert force in large degrees of an athlete’s range of movement (ROM). This can be seen in suplexes in Greco-Roman wrestling (132), throws in Judo (47), bridges in Swiss wrestling (133) and shooting for takedowns in BJJ and freestyle wrestling (69, 129). Biomechanical analysis of Greco-roman wrestling has shown that many trajectories from throws, takedowns and presses follow Circular and Helicoidal paths, resulting in hip and spinal rotation (67). Therefore, the IPW adopts the scorpion exercise to increase ROM in these areas. Neck mobilisations are also required as research has shown that neck strengthening reduces cervical injuries in combat sports (62) as well as sports-related concussions (61).
Potentiate
The potentiate stage aims to increase activity to maximal intensity in preparation for competition (98). This often includes techniques such as PAPE (99). This technique is primarily used to improve sports performance and the focus of the IPW is to reduce athlete injury. However, it has been shown that coaches and athletes perceive performance as a higher priority than injury prevention (94). Flinch’s (2006) (134) proposal of the Translating Research into Injury Prevention Practice Framework (TRIPP) states that only research adopted by sports participants, their coaches, and sporting bodies can prevent injuries. By including performance aspects in the IPW, compliance levels are anticipated to increase. The potentiate section of the IPW starts with plyometric exercises. Plyometric training in adolescents has also been evidenced to increase neural drive to the agonist’s muscles, reactive strength stretches, shorting cycle efficiency, fascicle length, and Vastus Lateralis pennation angle and aid in the development of muscle activation strategies (135, 136, 137). PAPE exercises such as plyometric press-ups have shown increases (4.9 %) in peak power output (138).
This section also includes partner contact drills. Wrestling and contact drills have also been recommended as injury prevention strategies for contact injuries in Rugby League and Union (139, 140). The IPW concludes with a partner reaction drill designed by the British wrestling team’s coaching staff. This involves grapplers performing takedown defensive and attacking movements as they react to their partner’s cues. Visual processing, visual fields, and visual reaction times are essential to the performance of numerous sports and play a role in athletic injuries (141, 142). The partnered drills also allow grapplers to raise their heart rate after an anticipated drop in the mobilise section.
Conclusion
This is the first evidence-based IPW for grappling sports and may act as a resource for coaches of all grappling arts. It provides athletes and coaches with a warm-up that can be performed before grappling practice and competition. The IPW will be embedded into the British Wrestling Association’s (BWA) coaching courses and as a continuous professional development course (CPD) option for international grappling coaches. Further studies can be undertaken to verify the IPW effectiveness in reducing biomechanical injury risk factors, injury incident rates and performance benefits.
Appendix
Table 1. IPW with rationale and coaching points
| Evidence-based Injury Prevention Warm-up for Grappling Sports | ||
| Exercise | Rationale | Description and coaching points |
| Raise | ||
| Head circumduction (Walking) | Pulse-raising exercises – Research has recorded an average heart rate of 180 to 182 bpm in grappling matches and can reach a maximum of 190 – 200 (110, 111). High knees and heels-to-glutes exercises have been shown to increase dynamic mobility of the spine and peripheral joints (84) | The pulse-raising exercises can be performed in a line format down the wrestling mat (12 m) and back. The length and, therefore, duration of each exercise can be altered depending on the group’s ability levels. Grapplers should aim for full ROM in each exercise. |
| High knees (Jogging) | ||
| Heel to glutes (Jogging) | ||
| Stance side shuffles (Both directions) | ||
| Head rotations (Jogging) | ||
| Shoulder rolls (Jogging) | ||
| Forwards rolls (commando roll) | Rolling has been shown to increase proprioception and postural control (112, 113). | Grapplers will forward roll down the length of the mat. Then backwards roll back to the starting position. Forward rolls can be progressed into dive rolls, and backwards rolls can be progressed into backwards rolls to handstands, depending on athletic ability. |
| Backwards rolls | ||
| Shuffle sprints | Grapplers need the ability to produce a rate of force development and acceleration for movements such as takedowns (69). | Grapplers will shuffle sprint on the spot until a signal comes from the coach to sprint to the opposite end of the mat. This will be performed twice. |
| Activate | ||
| Walking Lunge with thoracic rotation. | Electromyography (EMG) research has demonstrated that forward lunges increased activation in the Vastus Mediali and gluteus Medius and have been used in peer-reviewed injury prevention and performance warm-ups (119, 120). | Slow, full ROM lunges with a trunk rotation. Along the length of the mat. |
| Bear Crawl | Bear crawls have been used in wrestling and functional training settings to activate the wrists, pelvis and lower limbs (121, 122). | Grapplers should maintain a degree of flexion in the elbow and knee joints. This can be progressed to chimp walks. |
| Wheelbarrow walks (partner drill) | The wheelbarrow position mimics wrestling positions that requires the grappler to support their body weight with their upper extremities (81). Research using EMG has shown that press-up variations such as the wheelbarrow exercise activated the lower trapezius and the serratus anterior (124). | |
| Hindu press ups | Press-ups have been demonstrated to increase upper body and core activation (125) and have been used effectively in injury prevention warm-ups (128). Hindu press-ups involve a large degree of trunk and hip flexion that mimics the 110 degrees of trunk/hip flexion seen in the biomechanical analysis of a sprawl (129). | This exercise can be regressed to being performed on the knees. Grapplers should aim for full hip/trunk flexion. 30 seconds, 2 sets (84) |
| Hindu Squats | The squat has been successfully used to lower injury prevention and increase performance in the FIFA 11 + protocol (8, 130). The Hindu squat also allows grapplers to move into greater degrees of knee flexion needed to perform movements such as the double leg takedown (147 degrees) (129). | Grapplers are to ensure that their fingertips sweep the floor for every repetition. 30 seconds, 2 sets (84) |
| Breakfalls | Research has shown that many head, neck and trunk injuries in BJJ are a result of landing (25). It has been recommended that increased training in landing techniques will aid in preventing landing and fall injuries as demonstrated in Judo (25,47,63) | |
| Mobilise | ||
| Inchworm walks | It has been shown that grappling requires athletes to exert force in large degrees of ROM. This can be seen in suplexes in Greco-roman wrestling (132), throws in Judo (47), bridges in Swiss wrestling (133) and shooting for takedowns in BJJ and freestyle wrestling (129, 120) | These exercises will be executed in the line format used in the Raise section. Athletes will perform the exercises whilst advancing forward down the mat. The inchworm walks can be regressed to flexed knees for grapplers with reduced mobility. |
| RDL Walks | ||
| Laying Scorpions | Biomechanical analysis of Greco-roman wrestling has shown that many trajectories from throws, takedowns and presses follow Circular and Helicoidal paths, resulting in spinal rotation (67). | 10 repetitions on each side. (Clockwise and anti-clockwise). |
| Neck rolls | Neck strengthening has been shown to reduce cervical injuries in MMA (62) as well as sports-related concussions (61). | The Grapplers will place their hands and heads on the floor in a tripod shape. The grapplers will be knelt, leaning their weight into their heads. The grapplers will move their heads into flexion and extension, creating a rolling motion of their heads on the mat. This can be progressed by removing the support of the hands or by moving off the knees onto the feet. 20 repetitions for flexion into extension and 20 repetitions for lateral flexion. |
| Potentiate | ||
| 360-degree bunny hops | Plyometric training in adolescents has also been evidenced to increase neural drive to the agonist’s muscles, reactive strength stretches, shorting cycle efficiency, fascicle length, and Vastus Lateralis pennation angle and aid in the development of muscle activation strategies (135, 136, 13). | Grapplers will advance down the length of the mat while performing bunny hops in a circular clockwise motion. Grapplers can perform as many bunny hops as necessary to complete a 360-degree rotation. |
| Broad Jumps | Grapplers will perform broad jumps towards the other side of the mat. Grapplers will perform as many horizontal jumps as necessary to reach the end of the mat (12m). | |
| Hurdle jumps | Grapplers will advance in a line towards the other side of the mat. Roughly every 3 metres, the grapplers will perform a knees-to-chest jump as in mimicking jumping over a hurdle. | |
| Double-leg takedown shoots | Grapplers will perform a double-leg takedown shoot. Alternating the lead leg for each shot. | |
| PLYO press-ups | ~ 4.9 % increases in PPO post-PLYO after 8 min (138) | The plyometric press-up can be performed in a standard press-up position or from the knee. 1 × 10 |
| Partner drills (Potentiate) | ||
| Pummelling | Partner contact drills – Strength-based Wrestling and contact drills have also been recommended as an injury prevention strategy for contact injuries in Rugby League and Union (83, 86, 140). Partner-based contact drills have also been successful in the FIFA 11+ injury prevention programme aimed at footballers (8). | 60 secs of pummelling |
| Arm drags | 5 arm drags on each side | |
| Partner pushes | Two grapplers will stand facing each other with their arms on each other’s shoulders at arm’s length (so flexion in the elbow joint is allowed). The first grappler will then push the other down the length of the mat, and the grappler being pushed will give slight resistance and dictate circular angles to mimic a grappling bout. Once at the end of the mat (12 m), the grapplers will change roles. | |
| Double-leg takedown shoot with partner resistance. | Grapplers will start in the same position as the partner push. However, this time, grapplers will shoot a double-leg takedown, moving their partner backwards a few paces. The grappler will then stand back up rather than completing the takedown. This will be repeated until the end of the mat is reached. | |
| Partner reaction drill (Sudron drill) | Visual processing, visual fields, and visual reaction times are essential to the performance of numerous sports and play a role in athletic injuries (141). The partnered drills also allow grapplers to raise their heart rate after a possible drop in the mobilise section. | Reaction game: The grappler will start facing their partner, waiting for their signals. Both head in the air: The grappler will shoot a double leg takedown but not complete the takedown as practised in the partner shooting drill previously. Both hands down, pointing at the feet: The grappler will perform a spawl. One arm pointing at a leg: The grappler will move the leg back in a defensive motion. The time limit is 60 seconds for each grappler. |
- Jäggi U, Joray C, Brülhart Y, Luijckx E, Rogan S. Injuries in the martial arts judo, taekwondo and wrestling-a systematic review. Sportverletzung Sportschaden: Organ der Gesellschaft fur Orthopadisch-traumatologische Sportmedizin. 2015;29(4):219-225. [Link]
- Blach W, Smolders P, Simenko J, Mackala K. Diagnostics of tissue involved injury occurrence of top-level judokas during the competition: Suggestion for prevention. PeerJ. 2022;10:e13074. [Link]
- Powell JR, Boltz AJ, Robison HJ, Morris SN, Collins CL, Chandran A. Epidemiology of Injuries in National Collegiate Athletic Association Men’s Wrestling: 2014–2015 Through 2018–2019. Journal of Athletic Training. 2021;56(7):727-733. [Link]
- Pierantozzi E, Muroni R. Judo high-level competition injuries. MEDITERRANEAN JOURNAL OF SURGERY AND MEDICINE. 2009;17:26-29. [Link]
- Lopes J, de Magalhães Neto AM, Ferreira G, de Almeida AC, Andrade C. Etiology, prevalence, and severity of reported acute sports injuries in Brazilian Jiu-Jitsu Paradesports: an observational study. Science & Sports. 2021;36(2):e43-e50. [Link]
- Coppack RJ, Etherington J, Wills AK. The effects of exercise for the prevention of overuse anterior knee pain: a randomized controlled trial. The American journal of sports medicine. 2011;39(5):940-948. [Link]
- LaBella CR, Huxford MR, Grissom J, Kim K-Y, Peng J, Christoffel KK. Effect of neuromuscular warm-up on injuries in female soccer and basketball athletes in urban public high schools: cluster randomized controlled trial. Archives of pediatrics & adolescent medicine. 2011;165(11):1033-1040. [Link]
- Barengo NC, Meneses-Echávez JF, Ramírez-Vélez R, Cohen DD, Tovar G, Correa Bautista JE. The impact of the FIFA 11+ training program on injury prevention in football players: a systematic review. International journal of environmental research and public health. 2014;11(11):11986-12000. [Link]
- O’Brien J, Finch CF, Pruna R, McCall A. A new model for injury prevention in team sports: the Team-sport Injury Prevention (TIP) cycle. Science and Medicine in Football. 2019;3(1):77-80. [Link]
- Bell D, Travis, Jones. A. Injury Incidence and Prevalence in a Sample of Wrestlers Based in Britain: A Retrospective Study. Journal of Elite Sport Performance. 2023;3. [Link]
- Scoggin III JF, Brusovanik G, Izuka BH, Zandee van Rilland E, Geling O, Tokumura S. Assessment of injuries during Brazilian jiu-jitsu competition. Orthopaedic journal of sports medicine. 2014;2(2):2325967114522184. [Link]
- Kreiswirth EM, Myer GD, Rauh MJ. Incidence of injury among male Brazilian jiujitsu fighters at the World Jiu-Jitsu No-Gi Championship 2009. Journal of athletic training. 2014;49(1):89-94. [Link]
- Agel J, Ransone J, Dick R, Oppliger R, Marshall SW. Descriptive epidemiology of collegiate men’s wrestling injuries: National Collegiate Athletic Association Injury Surveillance System, 1988–1989 through 2003–2004. Journal of athletic training. 2007;42(2):303. [Link]
- Yard EE, Collins CL, Dick RW, Comstock RD. An epidemiologic comparison of high school and college wrestling injuries. The American Journal of Sports Medicine. 2008;36(1):57-64. [Link]
- Otero JE, Graves CM, Bollier MJ. Injuries in collegiate wrestlers at an elite Division I NCAA wrestling program: an epidemiological study. The Iowa orthopaedic journal. 2017;37:65. [Link]
- Kroshus E, Utter AC, Pierpoint LA, et al. The first decade of web-based sports injury surveillance: descriptive epidemiology of injuries in US high school Boys’ wrestling (2005–2006 through 2013–2014) and National Collegiate Athletic Association Men’s wrestling (2004–2005 through 2013–2014). Journal of athletic training. 2018;53(12):1143-1155. [Link]
- Hinz M, Kleim BD, Berthold DP, et al. Injury patterns, risk factors, and return to sport in Brazilian jiu jitsu: a cross-sectional survey of 1140 athletes. Orthopaedic journal of sports medicine. 2021;9(12):23259671211062568. [Link]
- Silva Junior JNd, Kons RL, Dellagrana RA, Detanico D. Injury prevalence in Brazilian jiu-jitsu athletes: comparison between different competitive levels. Revista Brasileira de Cineantropometria & Desempenho Humano. 2018;20:280-289. [Link]
- Usuki H, Rosen A, Jawed-Wessel S, Grandgenett N, McGrath M. Injury History, Severity, and Medical Care for Athletes Participating in Brazilian Jiu-Jitsu. Journal of Athletic Training. 2017;52(6):S153. [Link]
- Nery LC, Junior CCP, Saragiotto BT, et al. Prevalence and Profile of Musculoskeletal Injuries in High-Performance Professional Brazilian Jiu-Jitsu Athletes. The Open Sports Sciences Journal. 2022;16(5):1-6. [Link]
- Barreto AP, da Silva WM, Santos NVS, et al. Evaluation of mechanisms and types of injuries in jiu-jitsu athletes. J Exerc Physiol. 2017;20(2):10-16. [Link]
- McDonald AR, Murdock Jr FA, McDonald JA, Wolf CJ. Prevalence of injuries during Brazilian jiu-jitsu training. Sports. 2017;5(2):39. [Link]
- Hunker JJ, Tarpada SP, Khoury J, Goch A, Kahn M. Injuries common to the brazilian jiu-jitsu practitioner. Cureus. 2023;15(4). [Link]
- de Almeida T, de Araújo A. Factors that Influence Injuries Occurrence in Jiu-Jitsu Competitors. Int J Sports Exerc Med. 2020;6:164. [Link]
- Stephenson C, Rossheim ME. Brazilian jiu jitsu, judo, and mixed martial arts injuries presenting to United States emergency departments, 2008–2015. The journal of primary prevention. 2018;39:421-435. [Link]
- Juliano Eustaquio JM, Fontoura Borges AM, Vilela LS, et al. Does the fight profile interfere with orthopedic injuries in Brazilian Jiu-Jitsu? Open access journal of sports medicine. 2021:171-178. [Link]
- Jarrett GJ, Orwin JF, Dick RW. Injuries in collegiate wrestling. The American journal of sports medicine. 1998;26(5):674-680. [Link]
- Agarwal S, Mann E. Knee Injuries in Wrestlers: A Prospective Study from the Indian Subcontinent. Asian J Sports Med. Dec 2016;7(4):e35000. doi:10.5812/asjsm.35000. [Link]
- Barroso BG, Silva JMAd, Garcia AdC, et al. Musculoskeletal injuries in wrestling athletes. Acta Ortopédica Brasileira. 2011;19:98-101. [Link]
- Błach W, Lapaeva AG, Tabakov SY, Stelmach P. Main causes of upper limb belt injuries in judo and sambo. Polish Journal of Sports Medicine. 2022;38(1):19-24. [Link]
- Sistar A, Minoonejad H, Alizadeh MH, Seyedahmadi M. Epidemiology of Injuries in Iranian Male Jiu-Jitsu Athletes. Journal of Preventive Medicine. 2023;10(2):118-129. [Link]
- Nicolini AP, Penna NA, Oliveira GTD, Cohen M. Epidemiology of orthopedic injuries in jiu-jitsu athletes. Acta Ortopédica Brasileira. 2021;29:49-53. [Link]
- Akhmedov R, Demirhan B, Clcioglu İ, Canuzakov K, Turkmen M, Gunay M. Injury by regions seen in greco-roman & freestyle wrestling. Turkish Journal of Sport and Exercise. 2016;18(3):99-107. [Link]
- Daneshmandi H, Zolghadr H, Sedaghati P. Comparing the musculoskeletal injuries between the professional greco-roman and freestyle wrestlers. Physical Treatments, University of Social Welfare and Rehabilitation Sciences. 2020;10(1):15-22. [Link]
- Sandeep U, Kuloor H. A comparative study on common injuries among the Greco roman and free style wrestlers among university wrestlers. Foot. 2017;5(6.45). [Link]
- Akbarnejad A, Sayyah M. Frequency of sports trauma in elite national level greco-roman wrestling competitions. Archives of trauma research. 2012;1(2):51. [Link]
- Mooren J, von Gerhardt AL, Hendriks IT, Tol JL, Koëter S. Epidemiology of Injuries during Judo Tournaments. Translational Sports Medicine. 2023;2023. [Link]
- Akoto R, Lambert C, Balke M, Bouillon B, Frosch K-H, Höher J. Epidemiology of injuries in judo: a cross-sectional survey of severe injuries based on time loss and reduction in sporting level. British journal of sports medicine. 2018 Sep;52(17):1109-1115. [Link]
- Boden BP, Lin W, Young M, Mueller FO. Catastrophic injuries in wrestlers. The American journal of sports medicine. 2002;30(6):791-795. [Link]
- das Graças D, Nakamura L, Barbosa FSS, Martinez PF, Reis FA, Oliveira-Junior SAd. Could current factors be associated with retrospective sports injuries in Brazilian jiu-jitsu? A cross-sectional study. BMC sports science, medicine and rehabilitation. 2017;9(1):1-10. [Link]
- Green CM, Petrou MJ, Fogarty‐Hover ML, Rolf CG. Injuries among judokas during competition. Scandinavian journal of medicine & science in sports. 2007;17(3):205-210. [Link]
- Miarka B, Dal Bello F, Brito CJ, et al. Injuries during a World Judo Championship: differences between sex, weight category and competition phase. International Journal of Performance Analysis in Sport. 2018;18(2):229-244. [Link]
- Maciejewski R, Pietkiewicz S. Epidemiology of judo injuries in senior and junior judoka. Scientific Review of Physical Culture. 2016;6(3):27-36. [Link]
- Nokhodchi N, Moavenafshari M. The relationship between anthropometric and physical fitness factors and sport injuries among Iran’s National Team of Youth Freestyle Wrestling. Iranian Journal of Health and Physical Activity. 2013;4(2):56-62. [Link]
- Sarro KJ, Lara JPR, Martins L, et al. Seasonal variation of strength and power magnitude and asymmetry, and injury profile of Brazilian jiu-jitsu athletes. Journal of Physical Education and Sport. 2022;22(6):1346-1355. [Link]
- Almeida GPL, de Souza VL, Sano SS, Saccol MF, Cohen M. Comparison of hip rotation range of motion in judo athletes with and without history of low back pain. Manual therapy. 2012;17(3):231-235. [Link]
- Lockhart R, Błach W, Angioi M, Ambroży T, Rydzik Ł, Malliaropoulos N. A Systematic Review on the Biomechanics of Breakfall Technique (Ukemi) in Relation to Injury in Judo within the Adult Judoka Population. International Journal of Environmental Research and Public Health. 2022;19(7):4259. [Link]
- Petrisor BA, Del Fabbro G, Madden K, Khan M, Joslin J, Bhandari M. Injury in Brazilian jiu-jitsu training. Sports Health. 2019;11(5):432-439. [Link]
- de Carvalho MAF, do Nascimento MA, Pinheiro VHT, et al. Injury profile and risk factors in a young high competitive population of judo athletes. Training. 2018;247:71-72. [Link]
- Thomas RE, Zamanpour K. lnjuries in wrestling: systematic review. The Physician and sportsmedicine. 2018;46(2):168-196. [Link]
- Wiegmann S, Felsenberg D, Armbrecht G, Dietzel R. Longitudinal changes in muscle power compared to muscle strength and mass. Journal of Musculoskeletal & Neuronal Interactions. 2021;21(1):13. [Link]
- Trombetti A, Reid K, Hars M, et al. Age-associated declines in muscle mass, strength, power, and physical performance: impact on fear of falling and quality of life. Osteoporosis international. 2016;27:463-471. [Link]
- Cond R. Armlock in the closed guard: kinematic consequences to the kinetics of the technical gesture. Педагогико-психологические и медико-биологические проблемы физической культуры и спорта. 2018;13(2 (eng)):6-16. [Link]
- Almeida TBCD, Dobashi ET, Nishimi AY, Almeida EBD, Pascarelli L, Rodrigues LMR. Analysis of the pattern and mechanism of elbow injuries related to armbar-type armlocks in jiu-jitsu fighters. Acta Ortopédica Brasileira. 2017;25:209-211. [Link]
- Giannicola G, Sacchetti FM, Greco A, Cinotti G, Postacchini F. Management of complex elbow instability. Musculoskeletal Surgery. 2010;94:25-36. [Link]
- Schreiber JJ, Warren RF, Hotchkiss RN, Daluiski A. An online video investigation into the mechanism of elbow dislocation. The Journal of hand surgery. 2013;38(3):488-494. [Link]
- Hayashi H, Anata K, Ishikawa Y. Elucidation of the causes of head injury in judo: Is being thrown in an unexpected condition the cause of head injury? Journal of Physical Education and Sport. 2022;22(5):1169-1176. [Link]
- Murayama H, Hitosugi M, Motozawa Y, Ogino M, Koyama K. Ukemi technique prevents the elevation of head acceleration of a person thrown by the judo technique ‘Osoto-gari’. Neurologia medico-chirurgica. 2020;60(6):307-312. [Link]
- Koshida S, Ishii T, Matsuda T, Hashimoto T. Biomechanics of the judo backward breakfall: Comparison between experienced and novice judokas. Archives of Budo. 2014;10:187-194. [Link]
- Ishikawa Y, Anata K, Hayashi H, Yokoyama T, Ono T, Okada S. Effects of different throwing techniques in judo on rotational acceleration of uke’s head. International Journal of Sport and Health Science. 2018;16:173-179. [Link]
- Garrett JM, Mastrorocco M, Peek K, van den Hoek DJ, McGuckian TB. The relationship between neck strength and sports-related concussion in team sports: a systematic review with meta-analysis. journal of orthopaedic & sports physical therapy. 2023;53(10):585-593. [Link]
- Liu J. Effect of strength training on neck injuries prevention in martial arts athletes. Revista Brasileira de Medicina do Esporte. 2022;28:521-524. [Link]
- Koshida S, Ishii T, Matsuda T, Hashimoto T. Kinematics of judo breakfall for osoto-gari: Considerations for head injury prevention. Journal of sports sciences. 2017;35(11):1059-1065. [Link]
- Cipriano N. A technical–tactical analysis of freestyle wrestling. The Journal of Strength & Conditioning Research. 1993;7(3):133-140. [Link]
- Tünnemann H, Curby DG. Scoring analysis of the wrestling from the 2016 Rio Olympic Games. International Journal of Wrestling Science. 2016;6(2):90-116. [Link]
- Fujiyama K, Yamashita D, Nishiguchi S, Ito M. Technical-tactical analysis of men’s wrestling: a case study of the 72nd National Athletic Meet of 2017 in Japan. Int J Wresl Sci. 2019;9:1-6. [Link]
- Sacripanti A. Biomechanical classification of wrestling standing techniques. 1988: 254-265. [Link]
- Levitsky A, Matveyev D, Potsipun A, Oshina O, Kholodkova O. Biomechanical classification of actions in wrestling. Theory and Practice of physical culture. 2017;(10):23-23. [Link]
- Yamashita D, Arakawa H, Wada T, et al. Whole-Body Mechanics of Double-Leg Attack in Elite and Non-elite Male Freestyle Wrestlers. Frontiers in sports and active living. 2020;2:58. [Link]
- Sell TC, Ferris CM, Abt JP, et al. Predictors of proximal tibia anterior shear force during a vertical stop‐jump. Journal of Orthopaedic Research. 2007;25(12):1589-1597. [Link]
- Bennett DR, Blackburn JT, Boling MC, McGrath M, Walusz H, Padua DA. The relationship between anterior tibial shear force during a jump landing task and quadriceps and hamstring strength. Clinical biomechanics. 2008;23(9):1165-1171. [Link]
- Phisitkul P, James SL, Wolf BR, Amendola A. MCL injuries of the knee: current concepts review. The Iowa orthopaedic journal. 2006;26:77. [Link]
- Laprade RF, Wijdicks CA. The management of injuries to the medial side of the knee. journal of orthopaedic & sports physical therapy. 2012;42(3):221-233. [Link]
- Elkin JL, Zamora E, Gallo RA. Combined anterior cruciate ligament and medial collateral ligament knee injuries: anatomy, diagnosis, management recommendations, and return to sport. Current Reviews in Musculoskeletal Medicine. 2019;12:239-244. [Link]
- Pasque CB, Hewett TE. A prospective study of high school wrestling injuries. The American journal of sports medicine. 2000;28(4):509-515. [Link]
- Jang T-R, Chang C-F, Chen S-C, Fu Y-C, Lu T-W. Biomechanics and potential injury mechanisms of wrestling. Biomedical Engineering: Applications, Basis and Communications. 2009;21(03):215-222. [Link]
- Yard EE, Comstock RD. A comparison of pediatric freestyle and Greco‐Roman wrestling injuries sustained during a 2006 US national tournament. Scandinavian journal of medicine & science in sports. 2008;18(4):491-497. [Link]
- IBJJF. General Competition Guidelines Competition Format Manual. In: Federation IBJJ, editor. 5.2 ed2021. [Link]
- Waldén M, Atroshi I, Magnusson H, Wagner P, Hägglund M. Prevention of acute knee injuries in adolescent female football players: cluster randomised controlled trial. Bmj. 2012;344. [Link]
- van Beijsterveldt AM, van de Port IG, Krist MR, et al. Effectiveness of an injury prevention programme for adult male amateur soccer players: a cluster-randomised controlled trial. British journal of sports medicine. 2012; 46(16):1114-8. [Link]
- Grindstaff TL, Potach DH. Prevention of common wrestling injuries. Strength & Conditioning Journal. 2006;28(4):20-28. [Link]
- von Gerhardt AL, Reurink G, Kerkhoffs GM, et al. Effectiveness of a judo-specific injury prevention programme: a randomised controlled trial in recreational judo athletes. British journal of sports medicine. 2023;57(8):450-456. [Link]
- Gianotti SM, Quarrie KL, Hume PA. Evaluation of RugbySmart: a rugby union community injury prevention programme. Journal of Science and Medicine in Sport. 2009;12(3):371-375. [Link]
- Bizzini M, Dvorak J. FIFA 11+: an effective programme to prevent football injuries in various player groups worldwide—a narrative review. British journal of sports medicine. 2015;49(9):577-579. [Link]
- Riva D, Bianchi R, Rocca F, Mamo C. Proprioceptive training and injury prevention in a professional men’s basketball team: a six-year prospective study. Journal of strength and conditioning research. 2016;30(2):461. [Link]
- Attwood MJ, Roberts SP, Trewartha G, England ME, Stokes KA. Efficacy of a movement control injury prevention programme in adult men’s community rugby union: a cluster randomised controlled trial. British journal of sports medicine. 2018;52(6):368-374. [Link]
- Minnig MC, Hawkinson L, Root HJ, et al. Barriers and facilitators to the adoption and implementation of evidence-based injury prevention training programmes: a narrative review. BMJ Open Sport—Exercise Medicine. 2022;8(3). [Link]
- Fokkema T, de Vos R-J, Bierma-Zeinstra SM, van Middelkoop M. Opinions, barriers, and facilitators of injury prevention in recreational runners. Journal of Orthopaedic & Sports Physical Therapy. 2019;49(10):736-742. [Link]
- Richmond SA, Donaldson A, Macpherson A, et al. Facilitators and barriers to the implementation of iSPRINT: a sport injury prevention program in junior high schools. Clinical journal of sport medicine. 2020;30(3):231-238. [Link]
- Donaldson A, Callaghan A, Bizzini M, Jowett A, Keyzer P, Nicholson M. A concept mapping approach to identifying the barriers to implementing an evidence-based sports injury prevention programme. Injury prevention. 2018 25(4):244-251. [Link]
- Padua DA, Frank B, Donaldson A, et al. Seven steps for developing and implementing a preventive training program: lessons learned from JUMP-ACL and beyond. Clinics in sports medicine. 2014;33(4):615-632. [Link]
- Dix C, Logerstedt D, Arundale A, Snyder-Mackler L. Perceived barriers to implementation of injury prevention programs among collegiate women’s soccer coaches. Journal of science and medicine in sport. 2021;24(4):352-356. [Link]
- O’Brien J, Santner E, Kröll J. Moving beyond one-size-fits-all approaches to injury prevention: evaluating how tailored injury prevention programs are developed and implemented in academy soccer. journal of orthopaedic & sports physical therapy. 2021;51(9):432-439. [Link]
- Bolling C, Barboza SD, Van Mechelen W, Pasman HR. Letting the cat out of the bag: athletes, coaches and physiotherapists share their perspectives on injury prevention in elite sports. British journal of sports medicine. 2020;54(14):871-877. [Link]
- Noyes FR, Barber Westin SD. Anterior cruciate ligament injury prevention training in female athletes: a systematic review of injury reduction and results of athletic performance tests. Sports health. 2012;4(1):36-46. [Link]
- DiStefano LJ, Padua DA, Blackburn JT, Garrett WE, Guskiewicz KM, Marshall SW. Integrated injury prevention program improves balance and vertical jump height in children. The Journal of Strength & Conditioning Research. 2010;24(2):332-342. [Link]
- Gomes Neto M, Conceição CS, de Lima Brasileiro AJA, de Sousa CS, Carvalho VO, de Jesus FLA. Effects of the FIFA 11 training program on injury prevention and performance in football players: a systematic review and meta-analysis. Clinical rehabilitation. 2017;31(5):651-659. [Link]
- Jeffreys I. Warm up revisited–the ‘RAMP’ method of optimising performance preparation. UKSCA Journal. 2006;6:15-19. [Link]
- Finlay MJ, Bridge CA, Greig M, Page RM. Upper-body post-activation performance enhancement for athletic performance: a systematic review with meta-analysis and recommendations for future research. Sports Medicine. 2022;52(4):847-871. [Link]
- Silva LM, Neiva HP, Marques MC, Izquierdo M, Marinho DA. Effects of warm-up, post-warm-up, and re-warm-up strategies on explosive efforts in team sports: A systematic review. Sports Medicine. 2018;48:2285-2299. [Link]
- Celebrini RG, Eng JJ, Miller WC, et al. The effect of a novel movement strategy in decreasing ACL risk factors in female adolescent soccer players: a randomized controlled trial. Clinical journal of sport medicine: official journal of the Canadian Academy of Sport Medicine. 2014;24(2):134. [Link]
- Colclough A, Munro AG, Herrington LC, McMahon J, Comfort P. The effects of a four week jump-training program on frontal plane projection angle in female gymnasts. Physical Therapy in Sport. 2018;30:29-33. [Link]
- Lindblom H, Waldén M, Carlfjord S, Hägglund M. Limited positive effects on jump-landing technique in girls but not in boys after 8 weeks of injury prevention exercise training in youth football. Knee surgery, sports traumatology, arthroscopy. 2020;28:528-537. [Link]
- Belcher S, Whatman C, Brughelli M, Borotkanics R. Short and long versions of a 12-week netball specific neuromuscular warm-up improves landing technique in youth netballers. Physical Therapy in Sport. 2021;49:31-36. [Link]
- Nuhu A, Jelsma J, Dunleavy K, Burgess T. Effect of the FIFA 11+ soccer specific warm up programme on the incidence of injuries: A cluster-randomised controlled trial. PLoS One. 2021;16(5):e0251839. [Link]
- Ding L, Luo J, Smith DM, et al. Effectiveness of warm-up intervention programs to prevent sports injuries among children and adolescents: A systematic review and meta-analysis. International Journal of Environmental Research and Public Health. 2022;19(10):6336. [Link]
- Thorborg K, Krommes KK, Esteve E, Clausen MB, Bartels EM, Rathleff MS. Effect of specific exercise-based football injury prevention programmes on the overall injury rate in football: a systematic review and meta-analysis of the FIFA 11 and 11+ programmes. British journal of sports medicine. 2017; 51(7):562-571. [Link]
- Silvers-Granelli H, Mandelbaum B, Adeniji O, et al. Efficacy of the FIFA 11+ injury prevention program in the collegiate male soccer player. The American journal of sports medicine. 2015;43(11):2628-2637. [Link]
- Jeffreys I. RAMP warm-ups: more than simply short-term preparation. Prof Strength Cond. 2017;44:17-23. [Link]
- Degoutte F, Jouanel P, Filaire E. Energy demands during a judo match and recovery. British journal of sports medicine. 2003;37(3):245-249. [Link]
- Hernández-García R, Torres-Luque G, Villaverde-Gutierrez C. Physiological requirements of judo combat. International SportMed Journal. 2009;10(3):145-151. [Link]
- Anderson N, Button C, Lamb P. The effect of educational gymnastics on postural control of young children. Frontiers in Psychology. 2022;13:936680. [Link]
- Seyedi M, Zarei M, Daneshjoo A, et al. Effects of FIFA 11+ warm-up program on kinematics and proprioception in adolescent soccer players: a parallel‑group randomized control trial. Scientific Reports. 2023;13(1):5527. [Link]
- Markström JL, Olsson C-J. Countermovement jump peak force relative to body weight and jump height as predictors for sprint running performances:(in) homogeneity of track and field athletes? The Journal of Strength & Conditioning Research. 2013;27(4):944-953. [Link]
- Fradkin AJ, Zazryn TR, Smoliga JM. Effects of warming-up on physical performance: a systematic review with meta-analysis. The Journal of Strength & Conditioning Research. 2010;24(1):140-148. [Link]
- Kraemer WJ, Vescovi JD, Dixon P. The physiological basis of wrestling: Implications for conditioning programs. Strength & Conditioning Journal. 2004;26(2):10-15. [Link]
- Andreato LV, de Moraes SF, de Moraes Gomes TL, Esteves JDC, Andreato TV, Franchini E. Estimated aerobic power, muscular strength and flexibility in elite Brazilian Jiu-Jitsu athletes. Science & Sports. 2011;26(6):329-337. [Link]
- Jönhagen S, Ackermann P, Saartok T. Forward lunge: a training study of eccentric exercises of the lower limbs. The Journal of Strength & Conditioning Research. 2009;23(3):972-978. [Link]
- Daneshjoo A, Mokhtar A, Rahnama N, Yusof A. The effects of injury prevention warm-up programmes on knee strength in male soccer players. Biology of sport. 2013;30(4):281-288. [Link]
- Stastny P, Tufano JJ, Lehnert M, et al. Hip abductors and thigh muscles strength ratios and their relation to electromyography amplitude during split squat and walking lunge exercises. 2015;45(2):51-59. [Link]
- Childs E. Wrestling with the Truth, Part II. International Journal of Athletic Therapy and Training. 2001;6(5):36-36. [Link]
- Hernández-Lougedo J, Cimadevilla-Pola E, Fernández-Rodríguez T, et al. Effects of introducing rest intervals in functional fitness training. Applied Sciences. 2021;11(20):9731. [Link]
- Cumps E, Verhagen E, Meeusen R. Efficacy of a sports specific balance training programme on the incidence of ankle sprains in basketball. Journal of sports science & medicine. 2007;6(2):212. [Link]
- Andersen CH, Zebis MK, Saervoll C, et al. Scapular muscle activity from selected strengthening exercises performed at low and high intensities. The Journal of Strength & Conditioning Research. 2012;26(9):2408-2416. [Link]
- Gouvali MK, Boudolos K. Dynamic and electromyographical analysis in variants of push-up exercise. The Journal of Strength & Conditioning Research. 2005;19(1):146-151. [Link]
- Youdas JW, Budach BD, Ellerbusch JV, Stucky CM, Wait KR, Hollman JH. Comparison of muscle-activation patterns during the conventional push-up and perfect· pushup™ exercises. The Journal of Strength & Conditioning Research. 2010;24(12):3352-3362. [Link]
- Snarr RL, Esco MR. Electromyographic comparison of traditional and suspension push-ups. Journal of human kinetics. 2013;39:75. [Link]
- McCrary JM, Ackermann BJ, Halaki M. A systematic review of the effects of upper body warm-up on performance and injury. British journal of sports medicine. 2015;49(14):935-942. [Link]
- Denning. Wrestling: Biomechanics and Related Injuries. Sports Medicine Center: The Children’s Mercy Hospital. Accessed 10/12/2023, 2023. [Link]
- Hwang J, Kim J, Hwang J, Kim J. Effect of FIFA 11+ training program on soccer-specific physical performance and functional movement in collegiate male soccer players: A randomized controlled trial. Exercise Science. 2019;28(2):141-149. [Link]
- Koshida S, Matsuda T. Neck and Trunk Kinematics and Electromyographic Activity during Judo Backward Breakfalls. 2012. [Link]
- Hoffmann J, Amici C, Minelli C, Borboni A. Biomechanics of suplex in Greco-Roman wrestling: a qualitative and time-motion analysis of international competitions. International Journal of Performance Analysis in Sport. 2023;23(1):1-14. [Link]
- Lorenzetti S, Oberhofer K, Löhrer M, Lüthy F. BIOMECHANICAL ANALYSIS OF SCHWINGEN (SWISS WRESTLING) TO GAIN INSIGHTS INTO HEAD, NECK AND KNEE INJURY RISKS. ISBS Proceedings Archive. 2020;38(1):308. [Link]
- Finch C. A new framework for research leading to sports injury prevention. Journal of science and medicine in sport. 2006;9(1-2):3-9. [Link]
- Chmielewski TL, Myer GD, Kauffman D, Tillman SM. Plyometric exercise in the rehabilitation of athletes: physiological responses and clinical application. Journal of Orthopaedic & Sports Physical Therapy. 2006;36(5):308-319. [Link]
- Miller MG, Cheatham CC, Patel ND. Resistance training for adolescents. Pediatric Clinics. 2010;57(3):671-682. [Link]
- Secomb JL, Farley OR, Nimphius S, Lundgren L, Tran TT, Sheppard JM. The training-specific adaptations resulting from resistance training, gymnastics and plyometric training, and non-training in adolescent athletes. International Journal of Sports Science & Coaching. 2017;12(6):762-773. [Link]
- Ulrich G, Parstorfer M. Effects of plyometric versus concentric and eccentric conditioning contractions on upper-body postactivation potentiation. International journal of sports physiology and performance. 2017;12(6):736-741. [Link]
- Gabbett TJ, Jenkins DG, Abernethy B. Influence of wrestling on the physiological and skill demands of small-sided games. The Journal of Strength & Conditioning Research. 2012;26(1):113-120. [Link]
- Hollander SD, Ponce C, Lambert M, Jones B, Hendricks S. Tackle and ruck technical proficiency in rugby union and rugby league: A systematic scoping review. International Journal of Sports Science & Coaching. 2021;16(2):421-434. [Link]
- Clark J, Betz B, Borders L, Kuehn-Himmler A, Hasselfeld K, Divine J. Vision training and reaction training for improving performance and reducing injury risk in athletes. Journal of Sports and Performance Vision. 2020;2(1):e8-e16. [Link]
- Swanik CB, Covassin T, Stearne DJ, Schatz P. The relationship between neurocognitive function and noncontact anterior cruciate ligament injuries. The American journal of sports medicine. 2007;35(6):943-948. [Link]

